Infectious Deseases
Basic Research
Surveillance
Information
- Details
7th meeting of the COVID-19 advisory board of Ministry of Health, Labour and Welfare (September 1st, 2020).
Recent infection status, etc. (as of September 1st, 2020)
Trends in the number of new infections
- Infections by the time of onset appear to have reached a peak at the end of July across the country, and the effective reproduction number in all major cities is recently below 1.
- New infections are showing a slight decrease across the country, possibly owing to active measures in high-risk places such as night clubs and similar entertainment establishments where food and beverages are served, cooperation with a request for self-restraint by prefectural governments, and changes in the behavior of citizens; however, the trend in the number of infections varies between regions.
Cumulative number of infections per 100,000 people for one week (August 25 to 31): 4.13 (5,209↓) nationwide, 9.98 (1,389↓) in Tokyo, 4.05 (306↓) in Aichi, 7.36 (648↓) in Osaka, 8.41 (429↓) in Fukuoka, and 15.97 (232↓) in Okinawa
Rate of cases of unknown infection route (August 22 to 28): 50.8% (0.1%↓ from previous week) nationwide, 59.5% (2.4%↓) in Tokyo
Trends in the number of inpatients (*)
- The number of inpatients is decreasing slightly, though it is at a high level. The ratio of the number of inpatients to the number of available beds (in parenthesis) shows a similar trend; it is increasing in some regions in particular and remains high.
・Number of inpatients (August 26): 5,581↓ (24.5%) nationwide, 1,588↓ (48.1%) in Tokyo, 369↑ (46.6%) in Aichi, 483↓ (38.4%) in Osaka, 272↓ (55.5%) in Fukuoka, and 289 ↓ (62.7%) in Okinawa - The number of patients with severe disease has been increasing from early July; however, it is at a similar level to that during the previous week and has not reached the peak that was seen around April (381 [April 28]).
・Number of patients with severe disease (August 26): 331 (274↓) (11.5% [9.6%]*) nationwide, 83 (43↓) (20.8% [10.5%]*) in Tokyo, 21↑ (30.0%) in Aichi, 72↑ (38.3%) in Osaka, 16↓ (26.7%) in Fukuoka, and 24↓ (49.0%) in Okinawa
Test system
- Although the number of tests fluctuated, the rate of positive test results to the most recent number of tests is 4.0%, which decreased by 0.3% points from the previous week and remains low compared to that under the state of emergency (8.8% from April 6 to 12).
・Number of tests (August 24 to 30): 133,493↓ nationwide, 36,090↓ in Tokyo, 4,707↓ in Aichi, 10,634↓ in Osaka, 8,878↓ in Fukuoka, and 2,632↓ in Okinawa
・Rate of positive test results (August 24 to 30): 4.0% (0.3% points↓ from previous week) nationwide, 3.8% (0.3% points↓) in Tokyo, 6.5% (1.9% points↓) in Aichi, 6.2% (0.9% points) ) in Osaka, 5.1% (0.5% points ↑) in Fukuoka, and 8.8% (1.8% points↑) in Okinawa
- Details
9th meeting of the COVID-19 advisory board of Ministry of Health, Labour and Welfare (September 24, 2020). Document 3
Recent infection status
Trends in the number of new infections
- Infections by time of onset nationwide are decreasing from the peak seen at the end of July, but this trend appears to have slowed down. Since the last week of August, the effective reproduction number in Tokyo, Osaka, and Aichi has remained approximately 1, and the latest nationwide number is also close to 1.
- New infections were showing a decrease nationwide, possibly owing to active measures in high-risk places such as night clubs and similar entertainment establishments where food and beverages are served, cooperation with the request for self-restraint by prefectural governments, and changes in the behavior of citizens; however, the number of new infections is showing a slight increase and attention should be paid to this trend.
▪ Cumulative number of infections per 100,000 population for one week (September 9 to 15 and 16 to 22): 2.96 (3,731↑) and 2.61 (3,287↓) nationwide, 9.02 (1,255↑) and 8.05 (1,120↓) in Tokyo, 2.79 (211↑) and 2.52 (190↓) in Aichi, 6.37 (561↑) and 5.04 (444↓) in Osaka, and 2.27 (116↓) and 0.92 (47↓) in Fukuoka
▪ Rate of cases with unknown infection route (September 12 to 18): 48.4% (0.5%↓ from previous week) nationwide, 50.5% (3.5%↓) in Tokyo
Trends in the number of inpatients (*)
- The number of inpatients is showing a decreasing tendency. The ratio of the number of inpatients to the number of available beds (in parentheses) is similar, but slightly higher in some regions.
・Number of inpatients (September 16): 3,754↓ (14.2%) nationwide, 1,234↓ (30.9%) in Tokyo, 172↓ (21.7%) in Aichi, 375↓ (28.3%) in Osaka, 144↓ (29.4%) in Fukuoka, and 145↓ (31.2%) in Okinawa - The number of patients with severe disease has been increasing from early July, but has been decreasing since late August onward.
・Number of patients with severe disease (September 16): 316 (300↓) (9.6% [9.1%]) nationwide, 116↑ (23.2%) in Tokyo, and 19↑ (27.1%) in Aichi,51 (35↓) (19.5% [13.4%]) in Osaka (*), 10↓ (16.7%) in Fukuoka, and 22↑ (41.5%) in Okinawa
Test system
- Although the number of tests has fluctuated, the rate of positive test results to the most recent number of tests is 2.9%, which remains low compared to that under the state of emergency (8.8% from April 6 to 12). However, attention should be paid to the influence of a decrease in the number of tests due to 4 consecutive holidays (Silver Week).
・Number of tests (September 7 to 13 and 14 to 20 [*]): 126,734↓ and 81,024↓ nationwide, 37,369↑ and 19,614↓ in Tokyo, 4,315↑ and 3,006↓ in Aichi, 9,986↓ and 6,409 in Osaka, and 6,652 ↓ and 4,899↓ in Fukuoka
・Rate of positive test results (September 7 to 13 and 14 to 20 [*]): 2.9% (0.1% points↓ from the previous week) and 4.3% (1.4% points↑) nationwide, 3.3% (0.5% points↑) and 6.1% (2.8% points↑) in Tokyo, 4.6% (0.4% points↓) and 6.9% (2.3% points ↑) in Aichi, 5.7% (1.2% points↓) and 7.2% (1.5% points↑) in Osaka, and 1.9% (1.0% points↓) and 1.2% (0.7 points↓) in Fukuoka
Concerning the number of patients with severe disease, the criteria for targets differ from those published on August 14 or earlier. ↑ represents an increase from the previous week, and ↓ represents a decrease.
*Concerning the number of patients with severe disease, the criteria for the targets differ from those published from September 16. The figures in parentheses represent comparison with the same criteria for the previous week.
*Numbers of tests between 9/14 and 20 are provisional, and do not include some results obtained from private laboratories and medical institutions. The rates of positive test results are also provisional since these figures were obtained by dividing the number of positive patients by the number of tests.
Evaluation of Recent Infectious Status
Infection status
- New infections have been decreasing from the peak seen nationwide in the first week of August, but this trend appears to have slowed down. The epidemic curve based on the date of onset has shown a downward trend from the peak seen on July 27 to 29, but this trend has slowed down. The rate of positive test results decreased by 0.1% points from the previous week to 2.9%. (during the week of September 13)
- Since the first week of August, new infections have been decreasing, possibly due to active measures in high-risk places where spread of the infection may be triggered, such as night clubs and similar entertainment establishments where food and beverages are served, effective cooperation with the request for self-restraint by prefectural governments, and the effects of changes in the behavior of citizens who watch news reports on the spread of infection.
- On the other hand, since the last week of August, the decreasing trend in new infections has stopped and a slight increasing trend has been observed in multiple municipalities. Attention should be paid to these trends. In particular, the effective reproduction number in Tokyo, Osaka, and Aichi remains approximately 1 and the latest nationwide number is also close to 1. This suggests that the infection has spread through such opportunities as business dinners and workplace contacts as social activities are increasing. It is necessary to pay continuous attention to prevent the spread of infection nationwide, including the influence of increased movement of people during the Silver Week holidays and the influence of a decreased number of tests.
- The proportion of middle-aged and elderly people among infected patients has also been fluctuating at higher levels than in June and July, and continuous attention should therefore be paid. On the other hand, the number of patients with severe disease has been increasing from early July, and has turned to decrease from late August onward.
- It is necessary to note that the spread of infection continues around the world with approximately 300,000 new infections reported every day.
Future actions
- It is necessary to continue with active measures in high-risk places such as night clubs and similar entertainment establishments where food and beverages are served, where spread of the infection is triggered in Japan, and to reinforce measures against opportunities to develop cluster infections, including business dinners and workplace contacts. Movement of people and face-to-face social activities are expected to increase (e.g., holding of events, travel, resumption of on-campus classes). Therefore, the necessary measures should be thoroughly applied, e.g., basic preventive measures against infection such as avoiding the “3Cs” and environments where loud voices are raised, the wearing of masks indoors, keeping a proper physical distance, and thorough ventilation.
- It is also necessary to minimize the number of patients with severe disease and deaths by implementing measures against infection in hospitals/facilities for elderly people. The required measures should continuously be taken, including prompt actions against cluster outbreaks.
- On the other hand, spread of infection may be triggered in different places in the future, and it is required to organize a system of taking prompt and appropriate actions against large-scale clusters and cluster chains that may be the origin of infection spread in reference to overseas findings. It is also necessary to take note of possible unexpected re-spread in some regions.
Number of new infections (per 100,000 people) etc. (PDF)
- Details
Current Situation of COVID-19 Infection.
5th meeting of the COVID-19 advisory board of Ministry of Health, Labour and Welfare (August 6th, 2020).
Current Situation of Infection, August 5th, 2020.
Trends in the number of new infections
- The infection has continued to spread at restaurants with hospitality services, and through eating and drinking with friends and acquaintances, mainly in urban areas, but it is also spreading in rural areas.
- The number of new infections is increasing nationwide, and is increasing rapidly in some areas.
- Cumulative number of infected persons per 100,000 population per week (from July 30 through August 5)
Nationwide: 7.33 (9,248), Tokyo: 17.41 (2,424), Aichi: 14.38 (1,086), Osaka: 14.37 (1,266),
Fukuoka: 16.58 (846), Okinawa: 30.32 (439)
- Percentage of cases with unknown routes of infection (from July 25 through 31)
Nationwide: 52%, Tokyo: 59%
Trends in the number of hospitalized patients
- The number of inpatients is increasing, as is the ratio of the number of inpatients to the number of hospital beds secured for those patients (shown in parentheses).
- Number of inpatients (as of July 28; August 5 for Tokyo): Nationwide: 4,034 (20%), Tokyo: 1,475 (45%), Aichi: 195 (39%),
Osaka: 534 (42%), Fukuoka: 183 (37%), Okinawa: 83 (37%)
- On the other hand, the number of severely ill patients is currently low, but is gradually increasing. The ratio of the number of severely ill patients to the number of hospital beds secured for severely ill patients (shown in parentheses) is also gradually increasing.
- Number of severely ill patients (as of July 28; August 5 for Tokyo): Nationwide: 92 (4%), Tokyo: 21 (5%), Aichi: 2 (7%),
Osaka: 13 (7%), Fukuoka: 5 (8%), Okinawa: 2 (5%)
Test System
- In the last week, the number of test cases increased by 48%. The percentage of positive tests also increased to 6.7% (+0.7% points from the previous week), which is lower than when the state of emergency was declared (8.8% during the period from April 6 through 12); however, some local governments report a sharp increase.
- Number of tests (from July 27 through August 2): Nationwide: 127,700 (+48%), Tokyo: 32,605 (+36%), Aichi: 5,661 (+92%),
Osaka: 11,287 (+42%), Fukuoka: 10,312 (+95%), Okinawa: 3,433 (+143%)
- Percentage of positive tests (from July 27 through August 2): Nationwide: 6.7% (+0.7% points), Tokyo: 7.0% (-0.7% points),
Aichi: 18.5% (+3% points), Osaka: 11.1% (+1.4% points), Fukuoka: 7.4% (-0.3% points), Okinawa: 9.5% (+6.6% points)
- The average number of “onset-diagnosis days” declined, then leveled off.
- Average number of “onset-diagnosis days” (from July 13 through 19): Nationwide: 5.2, Tokyo: 5.2
*Mid-April (from April 13 through 19): Nationwide: 7.6, Tokyo: 9.0
Evaluation of the Current Situation of Infection
- Mainly in urban areas, the infection is continuing to spread at restaurants with hospitality services, and through eating and drinking with friends and acquaintances; however, the infection is also spreading in rural areas. The speed of the spread of infection is close to that observed in March and April due to its rapid spread in some areas, which is an alarming situation.
- On the other hand, since the infection is continuing to spread mainly among the younger generation, which differs from the situation in March and April, the ratio of hospitalized or severely ill patients remains low, compared to the number of infected people. However, the infection is gradually spreading to middle-aged persons and the elderly, and the number of severely ill patients is gradually increasing.
- With respect to the fact that the increase in the number of severely ill patients is moderate compared to the increase in the number of infected people, in addition to the increasing trend for infection among the younger generation, it is considered that early diagnosis has become possible, and treatments that contribute to the prevention of aggravation may have certain effects. However, at the present time, sufficient evidence has not been obtained and further analysis is required.
- With respect to the route of infection, etc., in those areas where there is an increasing number of infections, the proportion of infected persons with an unknown route of infection remains at a high level. Furthermore, infections in homes, medical institutions, elderly care facilities, etc. have continued to be reported.
- In addition, clusters have thus far been detected mainly in places such as restaurants with hospitality services, Japanese-style bars (Izakaya), and office meetings, where the “3Cs” (closed spaces, crowded places, and close contact settings) overlap and people talk in a loud voice.
- For the above reasons, in order to prevent the spread of infection, it is strongly required to continue to take basic infection control measures, such as avoiding environments where the “3Cs” overlap and people talk in a loud voice, wearing a mask indoors, thorough physical distancing, and thorough ventilation.
- At present, if such basic infection control measures are taken, it is unlikely that the infection will be spread via shopping at nearby supermarkets, using public transportation when commuting, working in the office, or the like.
- On the other hand, continued outbreaks and increases in the number of new infections have already adversely affected public health centers and medical institutions, and there are concerns regarding the tightness of the medical care provision system in some areas. This situation requires prompt measures to reduce the number of new infections, in order to reduce the burden on the public health system and the medical care provision system. This trend has been seen in some prefectures.
- It is necessary to continue to monitor and evaluate the situation of infection, and to promptly ensure a sufficient medical care provision system, for example, by expanding the number of hospital beds and securing accommodation and medical treatment facilities. In addition, if it is difficult to provide medical care using these facilities, based on the number of persons to be accepted, etc., it will be necessary to promptly inspect the status of the medical care provision system, including examination and development of a system to ensure that patients with mild symptoms or who are asymptomatic, and present a low risk of serious illness receive appropriate medical care at home (including the response when a patient’s physical condition deteriorates, as well as the provision of meals).
- Details
<Rapid report>Outbreak of novel coronavirus disease (COVID-19) on a cruise ship docked in Nagasaki City: preliminary interim report
Posted date 2020/6/3
In this report, we describe an outbreak of novel coronavirus disease (COVID-19) that occurred on the cruise ship, “Costa Atlantica”, docked in Nagasaki City, Nagasaki Prefecture. This report provides information pertaining to the confirmation of a cluster of COVID-19 cases, the initial test results, and the early situation on the ship. Response activities are currently ongoing, and this report should be considered as preliminary and interim.
On 29 January 2020, the Italian cruise ship, “Costa Atlantica”, entered Nagasaki Port and docked inside the port on 20 February, remaining there until 25 March for ship repairs. Since then, given the enhanced quarantine measures implemented globally, departure became difficult and the ship continued to remain in Nagasaki Port. All persons on the ship were crew members, with 623 persons on board on 20 April 2020. Many were young male adults; 523 (84%) were men with a median age of 31 years (range: 19-69 years). The majority were of foreign nationality, with the Philippines, India, Indonesia, and China (listed in descending order) contributing the largest number of crew members.
- Details
Descriptive epidemiology of 516 confirmed cases of novel coronavirus infection reported by the national epidemiological surveillance of infectious diseases (NESID) system and active epidemiological surveillance (as of March 23, 2020)
Posted date 2020/4/9
On February 1, 2020, novel coronavirus infectious disease (COVID-19) was added as a designated infectious disease under the Infectious Diseases Control Law, article 6 in paragraph 8, requiring physicians to immediately report diagnosed novel coronavirus infection cases to the public health center in their jurisdiction. Additionally, active epidemiological investigation became possible, as stipulated in the Infectious Diseases Control Law, article 15.
The primary sources of data in this report were lab-confirmed novel coronavirus infection cases (including asymptomatic SARS-CoV-2 infection cases) reported through both the National Epidemiological Surveillance of Infectious Diseases (NESID) system and the active epidemiological investigation program, as of March 23. Cases reported by local public health centers through NESID were linked to cases monitored daily for follow-up by members of the Novel Coronavirus Response Headquarters team at the Ministry of Health, Labour and Welfare (MHLW), via the active epidemiological investigation program. This report provides an update to the previous report for the data as of March 9 (https://www.niid.go.jp/niid/en/2019-ncov-e/2484-idsc/9497-covid19-14-200309-e.html), and is the third update thus far. As data collection is ongoing, the data may be revised or updated accordingly in the future. It should also be noted that there is delayed reporting or cases still in the process of notification for some cases. As such, there may be a difference in the number of cases in this report versus those officially reported by MHLW. It is expected that this difference will be gradually resolved in the future, but caution is required.
- Details
Descriptive epidemiology of 287 confirmed cases of new coronavirus infection reported by the national epidemiological surveillance of infectious disease system (NESID) and active epidemiological surveillance (as of March 9, 2020)
Posted date 2020/3/17
On February 1, 2020, new coronavirus infectious disease (COVID-19) was added as a designated infectious disease under the Infectious Diseases Control Law, article 6 in paragraph 8, which required doctors to immediately report diagnosed COVID-19 cases to the public health center in their jurisdiction. These reported cases were aggregated through the national epidemiological surveillance of infectious diseases (NESID) system. Additionally, active epidemiological investigation could then be conducted, as stipulated in the Infectious Diseases Control Law, article 15.
The primary sources of data in this report were lab-confirmed COVID-19 cases reported through NESID and active epidemiological investigations, as of March 9. Data in NESID were aggregated from reporting by local public health centers. Daily data in active epidemiological investigation by local public health centers were aggregated by teams from the Novel Coronavirus Response Headquarters at the Ministry of Health, Labor, and Welfare (MHLW). This updated report provides additions to the report published on February 24 (https://www.niid.go.jp/niid/en/2019-ncov-e/2484-idsc/9473-2019-ncov-08-e-2.html). As data collection is ongoing, this report may be revised or updated accordingly in the future. It should also be noted that there are cases in which there may have been delayed reporting or case notification not yet completed. As such, there may be a difference in the number of cases reviewed in this report versus those under active investigation by MHLW. It is expected that this difference will be resolved in the future, but please note that there may be a difference.
- Details
Descriptive epidemiology of 112 confirmed cases of novel coronavirus infectious disease (COVID-19) as reported by the national epidemiological surveillance of infectious diseases (NESID) system and active epidemiological investigation (as of February 24, 2020)
On February 1, 2020, the novel coronavirus infectious disease (COVID-19) was added as a designated infectious disease under the Infectious Diseases Control Law, article 6 in paragraph 8, which requires doctors to immediately report diagnosed COVID-19 cases to the public health center in their jurisdiction. These reported cases are aggregated through the national epidemiological surveillance of infectious diseases (NESID) system. Additionally, active epidemiological investigation can be conducted, as stipulated in the Infectious Diseases Control Law, article 15.
The primary sources of data in this report were lab-confirmed COVID-19 cases notified through NESID and active epidemiological investigations, as of February 24. Data in NESID are aggregated from reporting by local public health centers. Daily data in active epidemiological investigation by local public health centers were aggregated by teams from the Novel Coronavirus Response Headquarters at the Ministry of Health, Labor, and Welfare (MHLW). As data collection is ongoing, this report may be revised or updated accordingly in the future. It should also be noted that there are cases in which there may be delayed reporting or case notification has not been completed. As such, there may be a difference in the number of cases reviewed in this report versus those under active investigation by MHLW. It is expected that this difference will be resolved in the future, but please note that there may be a difference.
- Details
| February 27, 2020 | - Addition for the Implementation of Rapid Detection of Clusters (Populations) of Patients - |
| February 6, 2020 |
- Details
![]()
Case of First Human-to-Human Infection of Novel Coronavirus in Japan
The novel coronavirus (hereinafter, SARS-CoV-2) is a new type of coronavirus that has been detected in patients with pneumonia of unknown cause, which has occurred in Wuhan City, Hubei Province in the People's Republic of China since December 2019. On February 11, the World Health Organization (WHO) specified the official name for the novel coronavirus infection as “COVID-19 (coronavirus disease 2019)” (hereinafter referred to as “COVID-19”). This paper summarizes and reports the results of an active epidemiological surveillance forcases of human-to-human infection of COVID-19 in 3 persons with no travel history to Wuhan for 2 weeks before the onset of the disease, in cooperation with local governments.
Read more: Case of First Human-to-Human Infection of Novel Coronavirus in Japan
- Details
Field Briefing: Diamond Princess COVID-19 Cases, 20 Feb Update
Background:
Please refer to Field Brief: Diamond Princess COVID-19 Cases (https://www.niid.go.jp/niid/en/2019-ncov-e/9407-covid-dp-fe-01.html).
Quarantine Measures:
The initial quarantine period for those onboard the Diamond Princess was 5-19 February, with passengers informed that the 14-day quarantine could be extended if they were exposed to additional risk, for example close contact with a confirmed COVID-19 case. Additional details on quarantine measures can be found in “Field Briefing: Diamond Princess COVID-19”.
Disembarkation Procedures:
Criteria for disembarkation of non-cases from the Diamond Princess included 1) completion of a 14-day period without sharing a cabin with a confirmed case; 2) a negative result for a SARS-CoV-2 by PCR in the final days of the period; and 3) no relevant symptoms identified during a medical screening in the final day of the period. As of 20 February, over 1600 individuals have been disembarked from the Diamond Princess. Initially, testing focused on high-risk persons. Beginning on 11 Feb, efforts shifted toward testing all passengers by PCR for SARS-CoV-2. Due to the number of persons on board, these efforts began with passengers over 80, then over 75, then over 70, etc. After all passengers had been tested, the focus shifted to testing all crew members. Although no international guidelines require PCR testing to clear a quarantine for COVID-19 outbreaks, the Japanese government sought to do so as an additional measure of assurance.
Data Collection:
In addition the data collection methods described in Field Brief: Diamond Princess COVID-19 Cases; retrospective data collection has also begun by gathering information from the ship’s onboard clinic. Data here have been analysed descriptively.
Preliminary Results:
As of 20 February, 619 cases have been confirmed (16.7 % of the population on board), including 82 crew and 537 passengers. A total 3011 respiratory specimens were tested, and 621 were positive (20.6%), including double tests. Persons aboard between 70 and 89 were the most affected (Table 1). Among confirmed COVID-19 cases with recorded symptom onset (n=197), there were 34 (17.3 %) with onset dates before 6 February, which was the first full day of quarantine, and 163 (82.7%) with onset dates on or after the 6th (Figure 1). Among these 197 cases, 163 occurred during the quarantine period (48 crew, 115 passengers), with 52–92 among passengers in cabins without a previously confirmed case (Table 2). Of these, 3–7 occurred after the median quarantine day (day 7). The proportion of COVID-19 cases confirmed among passengers increased with cabin occupancy (Figure 2). A total 318 (51%) of all confirmed cases were asymptomatic when the respiratory specimen was collected (10 crew and 308 passengers).
Preliminary Conclusions:
Based on current available epidemiologic information, there is clear evidence that substantial transmission of SARS-CoV-2 was occurring prior to arrival of Diamond Princess in Yokohama. The subsequent decline in the number of confirmed cases with reported onset dates, may be explained by the natural course of the outbreak, by the implementation of quarantine measures, or by other unknown factors. Based on the cabin occupancy findings and the number of cases identified in cabins with previously confirmed cases, passengers within cabins may have been exposed to a common source or may have transmitted the virus within cabins. Due to the nature of the ship, individual isolation of all those aboard was not possible. Sharing cabins was necessary, and some crew had to perform essential duties while passengers remained aboard. After accounting for delayed reporting, the peak number of confirmed cases with known onset dates occurred on 7 February. The high number of recently reported cases can be explained by the shift in testing strategy described above, most of which were asymptomatic.
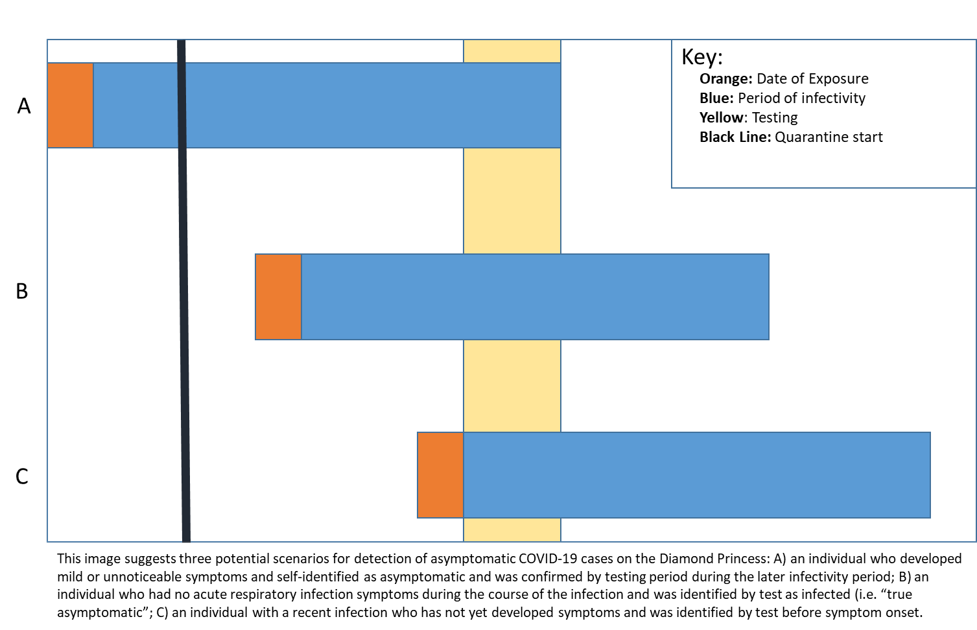
The proportion of asymptomatic cases observed aboard Diamond Princess is substantially higher than what has been reported elsewhere. A major factor in this proportion is the systematic testing of passengers that began on 11 Feb and increased each day. Due to the lack of symptom presentation, it is not possible to infer when these cases were infected (see Annex A). Some may have been secondary cases within a given cabin. Some may have been infected before the quarantine began. Nevertheless, these asymptomatic cases were detected through testing, disembarked, and transferred to isolation. Their cabin mates have been defined as close contacts with their 14-day isolation reset on the last day the asymptomatic case disembarked. The systematic testing of asymptomatic cases was therefore important and beneficial for identifying potentially infectious individuals before allowing them to disembark. Current global research has scant evidence on asymptomatic transmission of SARS-CoV-2; thus, ongoing efforts to thoroughly investigate asymptomatic cases from Diamond Princess will provide important information for the global COVID-19 outbreak. (Information on the development of symptoms after disembarkation of asymptomatic confirmed cases is being collected.)
Surveillance staff are working on merging the data from Diamond Princess with information from reported COVID-19 cases in the National Epidemiological Surveillance of Infectious Diseases (NESID) to understand more about the clinical presentation, severity and initial asymptomatic presentation. This information will be important for further the understanding this event and the global situation of COVID-19.
Preliminary Actions/Guidance:
Nearly all disembarked individuals have observed a 14-day quarantine without sharing a cabin with a confirmed case, have received a recent negative PCR-test, and have passed a medical screening for symptoms (e.g. fever, cough,). Individuals who shared a cabin with a confirmed case will be put in isolation until they complete a 14-day beginning after the last day of contact with a confirmed COVID-19 cabinmate. This includes a large proportion of the crew, who admirably performed essential tasks that allowed the quarantine to occur and should be appreciated for their service. As more than 1600 individuals, primarily passengers, have been disembarked from Diamond Princess, the focus and support will now shift toward preventing further transmission of SARS-CoV-2 among crew.
Although the disembarked persons have passed laboratory testing, medical screening and the 14-day quarantine, they are asked to stay at home, where feasible, 14 days unless absolutely necessary, as an additional precautionary measure. They are asked also to monitor themselves for symptoms and contact a a healthcare facility if symptoms develop.
Note: this work would not have been possible without the important efforts of medical teams who went aboard Diamond Princess to care for passengers and crew and obtain this necessary information; the efforts of the crew to provide essential services; and the collaboration of Princess Cruises.
Table 1. Percent of persons aboard confirmed with COVID-19 by age group and symptom status at the time of specimen collection. (As of 20 February).
|
Age group |
Symptomatic confirmed cases (%) |
Asymptomatic confirmed cases (%) |
Total confirmed cases (%) |
Persons aboard on 5 February |
|
00-09 |
0(0) |
1(6) |
1(6) |
16 |
|
10-19 |
2(9) |
3(13) |
5(22) |
23 |
|
20-29 |
25(7) |
3(1) |
28(8) |
347 |
|
30-39 |
27(6) |
7(2) |
34(8) |
428 |
|
40-49 |
19(6) |
8(2) |
27(8) |
334 |
|
50-59 |
28(7) |
31(8) |
59(15) |
398 |
|
60-69 |
76(8) |
101(11) |
177(19) |
923 |
|
70-79 |
95(9) |
139(14) |
234(23) |
1015 |
|
80-89 |
27(13) |
25(12) |
52(24) |
216 |
|
90-99 |
2(18) |
0(0) |
2(18) |
11 |
|
Total |
301(8) |
318(9) |
619(17) |
3711 |
Figure 1. Number of confirmed COVID-19 cases* with reported onset dates, by onset date, aboard Diamond Princess, 6 – 20 February 2020 (n=163)
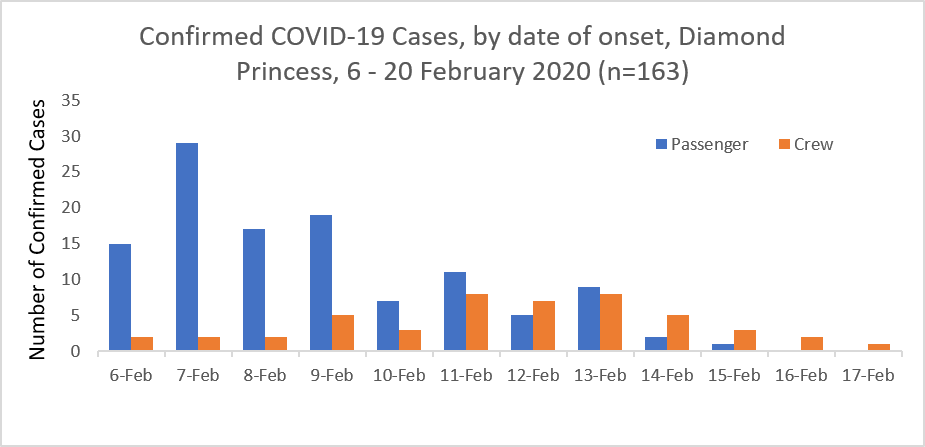
* The number of cases (n = 163) was based on the cases with available onset date reported.
Figure 2. Comparison of proportions of confirmed cases among passengers by cabin occupancy.
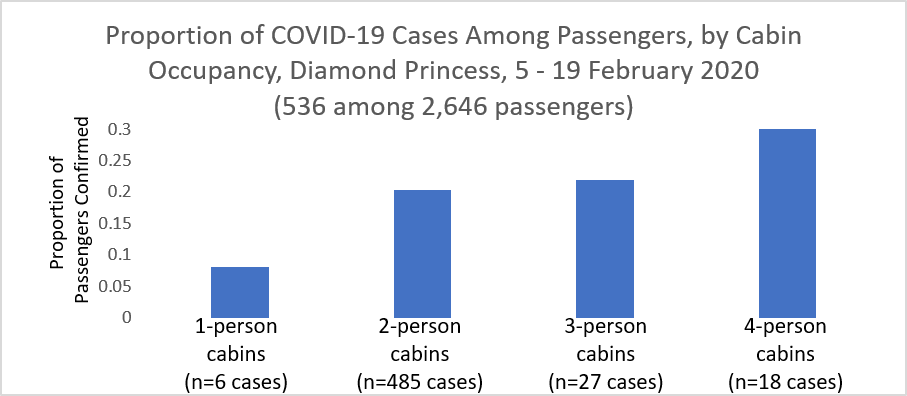
Table 2. Characteristics of COVID-19 Cases with reported on-set dates of 6 – 17 Feb 2020 (n=163).
|
Day of Quarantine |
Date of Onset (n cases) |
Crew |
Passengers |
||
|
Total |
In cabins with a confirmed case |
In cabins without a confirmed case |
|||
|
12 |
17 Feb (1) |
1 |
0 |
0 |
0 |
|
11 |
16 Feb (2) |
2 |
0 |
0 |
0 |
|
10 |
15 Feb (4) |
3 |
1 |
0 [1] |
0-1 |
|
9 |
14 Feb (7) |
5 |
2 |
1 [0] |
1 |
|
8 |
13 Feb (17) |
8 |
9 |
4 [3] |
2-5 |
|
7 |
12 Feb (12) |
7 |
5 |
0 [2] |
3-5 |
|
6 |
11 Feb (19) |
8 |
11 |
3 [1] |
7-8 |
|
5 |
10 Feb (10) |
3 |
7 |
3 [1] |
3-4 |
|
4 |
9 Feb (24) |
5 |
19 |
6 [9] |
4-13 |
|
3 |
8 Feb (19) |
2 |
17 |
1 [7] |
9-16 |
|
2 |
7 Feb (31) |
2 |
29 |
4 [10] |
15-25 |
|
1 |
6 Feb (17) |
2 |
15 |
1 [6] |
9-14 |
|
|
Total |
48 |
115 |
23 [40] |
52-92 |
The number in brackets represents the number of additional confirmed cases in the same cabin with unknown onset date. Due to the uncertainty of knowing which case came first, the column to the far right presents a range.
Annex A. Theoretical depiction of the identification of asymptomatic cases during the quarantine period.
- Details
Appreciation and Request from National Institute of Infectious Diseases, Japan
Dear Passenger,
We would like to extend our sincere gratitude for your patience and compliance in participating in the health observation period onboard the Diamond Princess from February 5th to 19th.
We would like to reassure you, based on your negative test results for the novel coronavirus and a successful medical visit confirming that you do not the fever or respiratory symptoms associated with the disease, that it is highly unlikely that you have been infected with the new coronavirus and can return to your normal lifestyle. We recognize that there may be concern for your health from many family and friends, so we would like to offer you the following guidance and requests from the National Institute of Infectious Diseases:
If you feel unwell during the next two weeks, please reach out for a consultation with the two institutes listed below:
- A visitor hotline operated by the Japan National Tourism Organization (JNTO)
http://www.mlit.go.jp/kankocho/content/001327108.pdf
(Support is available in English, Chinese and Korean)
- 日本語でのコミュニケーションが可能な方については、以下へのご相談が可能です。
(令和2年2月13日時点版)
https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/kenkou_iryou/covid19-kikokusyasessyokusya.html
In addition, as you have been carefully monitoring your health for the last two weeks, we would like to encourage you to continue with your usual disease prevention methods. This includes washing your hands often and wearing a mask.
We recognize that the recently disembarked passengers have been in the frontlines in the fight to prevent the invasion of emerging infectious diseases into Japan. We would like to request Japanese citizens for their maximum support in helping disembarked passengers regain their health and normal lifestyles.
February 21, 2020
National Institute of Infectious Diseases, Japan