118th Meeting of the COVID-19 Advisory Board of the Ministry of Health, Labour and Welfare (March 8, 2023) Material 1
Evaluation of the latest infection status, etc.
Overview of the infection status, etc.
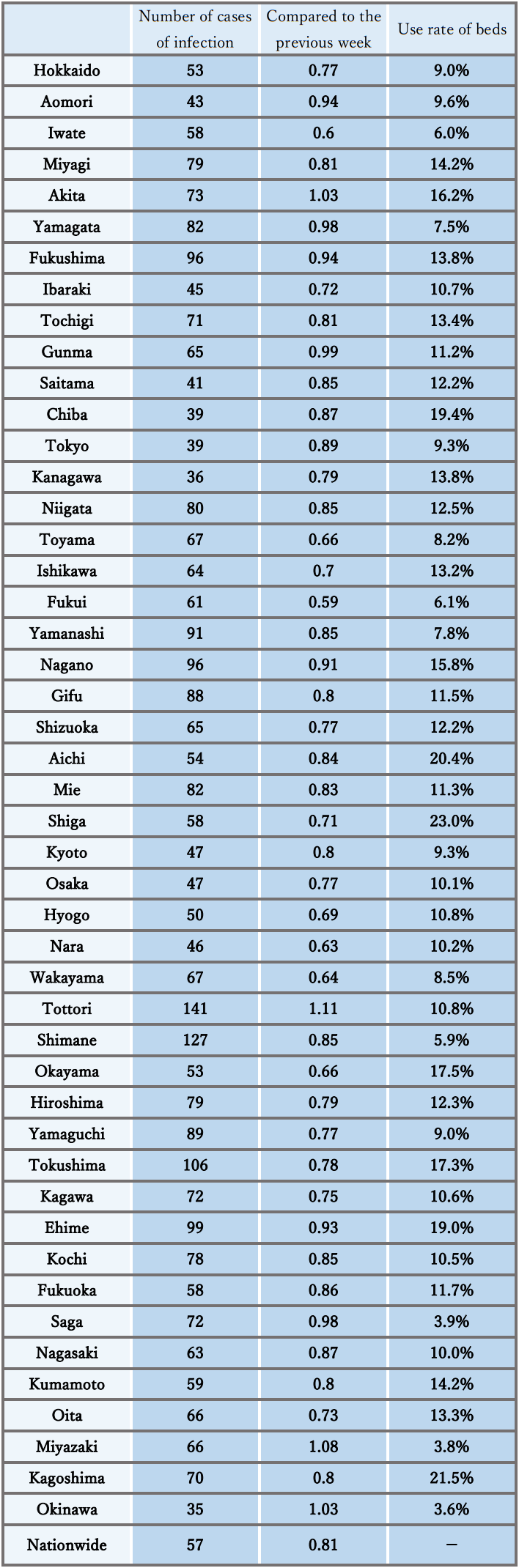
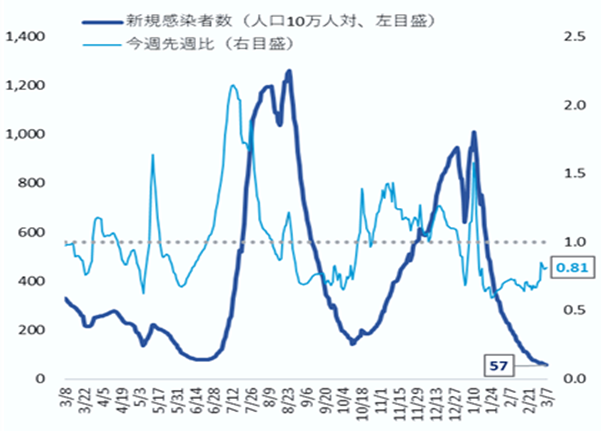
- The number of new cases of infection nationwide was approximately 57 per 100,000 of the population in the last week, showing a continuous decreasing trend with a ratio of this week to last week of 0.81.
It is necessary to pay attention to the future impacts of attenuation of immunity and replacement by variant strains on the infection status. - The use rate of beds has been decreasing nationwide, and the numbers of severe patients and deaths have also continued to decrease.
Reference: Local trend
*The number of new cases of infection is an approximate figure per 100,000 of the population, as the total for the current week, which is the reported number in HER-SYS as of Mar. 7, 00:00 AM (the same time point is used for the ratio to the previous week), and the use rate of beds is the secured bed use rate as of the time of writing this document on Mar. 7.
Infection status and future outlook
Infection status
- The number of new cases of infection shows a continuous decreasing trend nationwide, and the ratio to the previous week remains below 1.0 in most prefectures. The level is below that before the spread of infection in the summer of last year, and the decrease in the number of new cases of infection has been decreasing.
- Regarding the number of new cases of infection by region, in the Chugoku and Shikoku regions, the number per population is higher than the national average. Meanwhile, in the Kanto region and Okinawa, the number is lower than the average. In addition, there is a continuous decreasing trend in mass infections in facilities for elderly people, medical institutions, etc.
- The number of new cases of infection nationwide by age group shows a decreasing trend in all age groups, and the difference between age groups is smaller.
- The numbers of severe cases and deaths continue to show a downward trend nationwide. With the spread of infection this winter, the proportion of elderly patients in their 80s and older among newly infected patients tended to increase, compared to that during the spread of infection in the summer last year.
- As the reports of deaths among children since January 2022 suggest, attention must be paid to the occurrence of severe cases and deaths as well as the number of hospitalized children associated with an increase in the number of infected children.
- The incidence of seasonal influenza is lower than that during the same period of usual years, but higher than that during the same period of the last 2 years. At the time of announcement last weekend, the number of cases reported weekly per fixed-point medical institution had slightly decreased nationwide, compared to the previous week. But it is still at advisory level exceeding 10 nationwide, and at alert level exceeding 30 in Ishikawa, Iwate, and Fukui.
Future outlook
- Regarding the future infection status, it is expected that the number of new cases of infection will continue to be flat nationwide based on the epi curve and the short-term forecast nationwide and in large cities, although there are regional differences and uncertainty. In some regions, however, it may increase toward the end of March. It is necessary to pay attention to whether or not the increasing trend in regions with a ratio to the previous week of more than 1 will continue in the future, as well as the future impact of attenuation of immunity, an increase in the proportion of strains with potential to escape the immune system, and other factors on the infection status.
- The incidence of seasonal influenza is expected to continue to show a decreasing trend based on past trends, but attention should be paid continuously.
Factors that increase and suppress infection
- [Immunity as a result of vaccination and infection]
With the promotion of vaccination and natural infection, the proportion of immune carriers against the Omicron variant (BA.5 and BQ1.1) shows an increase in each age group, and it has been reported that the percentage is increasing particularly in the elderly population because of vaccination. However, immunity acquired from vaccination and natural infection may decline over time.
- [Contact status]
The nighttime population has been flat overall, although it has lately increased or decreased in some regions.
- [Epidemic strains]
Currently, the BA.5 lineage is the mainstream in Japan, but sublineages of the Omicron variant such as BQ.1 and XBB lineages, particularly XBB.1.5, which has been reported mainly in the US, are considered to have an enhanced ability to escape the immune system, and have been pointed out to predominate among the increasing number of infected people overseas. In Japan, the proportion of the BQ.1 lineage showed an increasing trend before but has been decreasing for 3 consecutive weeks. On the other hand, the proportion of the XBB.1.5 lineage seems to be increasing, and therefore attention needs to be paid. The proportion of the BN.1.3 lineage, which is a sublineage of the BA.2.75 lineage, has also been increasing in Japan.
- [Climatic and seasonal factors]
Days with low temperatures nationwide make ventilation difficult. Attention should also be paid to respiratory viral infections.
Situation of the medical care provision system
- The use rate of beds shows a decreasing trend nationwide and is at a low level below 30% in all regions. The use rate of beds for severe cases is also low nationwide.
- The number of patients receiving treatment in nursing care facilities has continued to decrease.
- In emergency medical care, the number of cases having difficulty with emergency transportation had been decreasing nationwide before but has been flat recently. Attention should continuously be paid to the future trend of the number of cases having difficulty with emergency transportation and securing a system to provide emergency medical care.
Measures to be taken
Basic concepts
- Unless we face special circumstances such as the emergence of a variant with a pathogenicity greatly different from that of the Omicron variant, COVID-19 shall be positioned as a Class V Infectious Disease instead of a Novel Influenza Infection, etc. under the Infectious Disease Act from May 8 this year (2023). In association with this, various policies and measures taken will be reviewed.
- Meanwhile, it is necessary to continue efforts to strengthen and focus the healthcare system to provide appropriate medical care for elderly people and those at high risk of aggravation, even with limited medical resources.
Each citizen will be asked to take voluntary actions to prevent infection to protect those at high risk of aggravation, such as elderly people, and to ensure regular medical care.
- 1. Further promotion of vaccination
- As for the “vaccine for the Omicron variant," vaccination of all persons aged 5 and older who have completed the first vaccination should proceed.
- As both vaccines for the BA.1 lineage and the BA.4 and BA.5 lineages are expected to be more effective than the previous vaccines, it is necessary to proceed with vaccination with either vaccine, whichever can be given sooner.
All eligible persons who wish to receive vaccination will be asked to receive the vaccine for the Omicron variant. - Those who have not received vaccination will be encouraged to consider getting the initial vaccination as soon as possible.
- For children (aged 5 to 11 years), the initial vaccination and additional vaccination with the vaccine for the Omicron variant will be promoted. For children (aged 6 months to 4 years), the initial vaccination will be promoted.
- Vaccination in FY 2023 will also be promoted (vaccination will be given to all eligible persons aged 5 years and older in autumn and winter, and additional vaccination will be given to elderly people and those at high risk of aggravation as well as spring and summer).
- 2. Use of tests
- The national and local governments are required to secure a system that enables testing, and should utilize testing.
- Perform frequent tests (about 2 or 3 times a week for facility workers) for workers at facilities for elderly people.
- Promote the establishment of a system for fever outpatients, whereby patients with symptoms can self-test using an antigen qualitative test kit, and if the result is positive, they can promptly undergo health observation at a health follow-up center, etc.
- Promote the utilization of antigen qualitative test kits, which have been switched to OTC and are sold on the Internet.
- 3. Quarantine measures
- Temporary measures have been taken for entrants from China from December 30 last year. The positive rate among entrants has been at a relatively low level, and all of the variants observed so far are lineages of the Omicron variant with a history of detection in Japan. Taking these accumulated findings and other circumstances into consideration, screening at the time of entry has been changed from testing of all entrants to sample testing of some entrants from March 1. Flexible responses will be given while observing the infection status in China, etc.
- 4. Securing a medical care provision system
With support of the national government, local governments are required to take measures to avoid overcrowding of hospital beds, fever clinics, etc.
- Maintain the total number of beds required for patients infected with COVID-19 based on the bed securing plan. In addition, continue to increase the number of medical institutions that can handle COVID-19 by supporting improvement of the ability to treat COVID-19 cases, even at hospitals without any beds for infected patients (promotion of zoning of hospital rooms, etc.).
- Take immediate responses such as securing beds, and make efforts to avoid being overwhelmed concerning the number of hospital beds and emergency medical care by using lodging facilities and resting beds, for example.
- Make appropriate adjustments so that patients who need hospital treatment can be hospitalized preferentially (securing and expanding logistical support hospitals, and improving the hospital turnover rate, such as by dissemination of the standard for early discharge of 4 days, as a rule). Implement frequent examinations at facilities for elderly people and others. Further strengthen medical support during normal times.
- In addition to extending the office hours and the number of outpatient clinics for fever patients, the outpatient medical care system is strengthened and prioritized by strengthening regional outpatient and testing centers and telephone and online clinics, etc.
- Local residents should be informed that they should refrain from visiting emergency outpatient units only to receive a precautionary examination if they do not have symptoms, for example, taking the actual situation in the region into consideration, so that nobody is prevented from receiving treatment. To respond to concerns and questions when a patient’s physical condition deteriorates, telephone consultation services by healthcare professionals should be thoroughly publicized, and this service should also be strengthened.
- 5. Response to simultaneous epidemics of COVID-19 and seasonal influenza
- The following efforts should be promoted according to the actual situation in each region: strengthening of the fever outpatient clinics, strengthening of telephone consultations/telemedicine, expansion of health follow-up centers, securing of self-test kits, strengthening of the consultation system, and prevention of overcrowded emergency medical care.
Smooth supply of medications including oral drugs prescribed after confirmation of the indication by physicians will be promoted. Pharmacies, etc. will be asked to use the consultation service of the Ministry of Health, Labour and Welfare when it is difficult to obtain antipyretic analgesics. - The prefectures will work to strengthen and prioritize the health care system based on plans to establish systems such as strengthening of outpatient medical care systems in accordance with the actual conditions in each region.
- It is necessary to provide information and send appropriate messages to the public depending on the infection status. People at low risk of aggravation will be encouraged to use a self-test kit or local follow-up center.
- People will be advised to do the following: check the “guide for ambulance services” in preparation for an acute illness or injury, consult a family doctor when hesitant to call an ambulance, use a telephone consultation service such as #7119, and call an ambulance without hesitation if necessary.
- At the same time, vaccination against COVID-19 and seasonal influenza of those who are subject to vaccination should be promoted.
- The following efforts should be promoted according to the actual situation in each region: strengthening of the fever outpatient clinics, strengthening of telephone consultations/telemedicine, expansion of health follow-up centers, securing of self-test kits, strengthening of the consultation system, and prevention of overcrowded emergency medical care.
- 6. Surveillance and risk assessment, etc.
- It is necessary to promptly promote consideration of effective and appropriate surveillance to grasp the epidemic status. It is also necessary to continue monitoring of the trends of variants through genomic surveillance.
- Regarding the risk assessment of COVID-19, it is necessary to continue evaluation of the pathogenicity, infectivity, mutations, etc.
- 7. Effective ventilation
- It is necessary to publicize and recommend effective ventilation methods to prevent insufficient indoor ventilation (how to create airflow considering aerosols and installation of partitions that do not block the airflow, for example) due to the use of heating appliances on days with low temperatures.
- 8. Re-inspection and implementation of basic infection control measures
Re-inspection and implementation of the following basic infection control measures are needed.
- Continue proper wearing of nonwoven masks according to the situation, hand hygiene, thorough ventilation, etc.
- Avoid situations with a high risk of infection, such as the three Cs, congestion, or loud voices.
- In the event of a meeting at a restaurant, choose a venue certified by a third party, keep the number of people as low as possible, avoid speaking in loud voices and staying for a long time, and wear a mask when talking.
- People with symptoms such as sore throat, cough, and fever should refrain from going out.
- Refer to guidelines for hospital visits and use of an ambulance.
- Prepare antigen qualitative test kits and antipyretic analgesics at home, and check the contact information of consultation services.
- Make efforts such as promoting the use of telework in the workplace.
- The organizers of events or meetings should examine and evaluate the epidemic status in the concerned region as well as the risk of infection, and then take measures to reduce the risk.
- From March 13 this year, the government will not uniformly request mask-wearing as a rule, but will respect the independent choice of individuals and leave the use of masks to their judgment. Until then, actions will be taken according to the previous policy.
- Test-positive persons on home care should monitor their own physical condition by such means as checking their body temperature and taking thorough measures against infection when going out. They must also be asked to avoid contact with people who are at risk of aggravation, such as elderly people.
- To allow the minimum necessary outings, such as shopping for groceries, after 24 hours have passed since symptoms have subsided or when there are no symptoms, it is necessary to take voluntary actions to prevent infection, such as wearing a mask when going out, keeping contact with other people at the minimum period of time possible, and not using public transportation.
<< Reference: Findings on the characteristics of the Omicron variant and its sublineages >>
- [Infectivity/transmissibility]
It has been confirmed that compared to the Delta variant, the generation time has shortened to approximately 2 days (approximately 5 days for Delta). The doubling time and incubation period have also shortened, the risk of re-infection and secondary infection after infection has increased, and the speed of infection spread is very fast. According to the reported data, pre-symptomatic transmission has probably occurred to some extent as with the previous strains.
- [Place/route of infection]
In Japan, many cases of infection have occurred through the same opportunities as before (spending time indoors in locations with inadequate ventilation, eating and drinking, etc.), and infection is also considered to have occurred via droplets adhering to mucosa, aerosol inhalation, contact infection, etc.
- [Severity, etc.]
It has been shown that infection with the Omicron variant may present a relatively lower risk of hospitalization or aggravation than with the Delta variant. To evaluate COVID-19, including the Omicron variant, it is not only necessary to assess the severity as a disease but also of the transmissibility and the impact on the medical care system and society as a whole.
Concerning the death toll since the outbreak at the end of 2021, it is reported that the novel coronavirus is not the direct cause of death in quite a number of cases compared to the epidemic in the summer of 2021; for example, when elderly people who had been living in a facility for elderly people since before the infection were infected and died, the death was due to worsening of the underlying disease. There were many cases of serious respiratory failure due to typical viral pneumonia caused by the novel coronavirus infection from the beginning of the novel coronavirus outbreak until the outbreak of the Delta variant. However, during the Omicron variant outbreak, it was reported that other diseases than pneumonia became the main causes of death, such as exacerbation of the underlying disease that had been present before hospitalization and the onset of other complications during hospitalization.
Concerning the spread of infection last summer, there has been a continuing decrease in the rate of severe cases and increase in the ratio of elderly people among hospitalized patients as during the previous outbreak compared to spreading of the infection in the summer of 2021. Among the deaths during the 2022 summer outbreak, mechanical ventilation/nasal high flow use rates and steroid prescription rates were decreased compared to the end of 2021 outbreak.
Among the fatal cases of infected children who died of endogenous factors, there were some cases without any underlying diseases. The reports on the results of on-site investigations have stated that it is necessary to pay attention to neurological symptoms such as convulsions and disturbance of consciousness, and systemic symptoms such as vomiting and poor oral intake besides the respiratory symptoms.
Among the deaths that occurred at home in July and August last year, approximately 80% of the patients were 70 years and older, which is similar to the trend of all deaths during the same period. It suggests that there were also many deaths caused by factors other than COVID-19. Regarding the situation of handling dead bodies known to be coronavirus positive, the number of cases reported monthly has been the highest during last December. The proportion of deaths due to COVID-19 has recently reached approximately 30% of all deaths.
- [Virus shedding period]
According to Japanese data, the risk of infection remains until 10 days after the onset, and infectivity is high until 7 days after the onset. Even after waiting for 5 days, a third of the patients are still shedding infectious viruses. On Day 8 (after isolation for 7 days), most patients (approximately 85%) did not shed infectious viruses, and it was reported that even if patients did shed the virus, the amount of virus decreased to one-sixth that in the initial stage of onset after 7 days.
- [Vaccine effects]
Concerning the conventional vaccine, the infection and disease onset prevention effects of the first vaccination against the Omicron variant are markedly reduced. The hospitalization-preventing effect is reported maintained at a certain level for the first 6 months, but subsequently decreases to 50% or less. On the other hand, it has been reported overseas that a third vaccination restores the infection-preventing, disease onset-preventing and hospitalization-preventing effects against infection with the Omicron variant, and information on how these vaccine effects are attenuated after a third vaccination has become available. Concerning the vaccine against the Omicron variant (BA.4-5), it has been reported that the preventive effect against disease onset was observed within 0 to 2 months (median 1 month) after vaccination.
- [Sublineages of the Omicron variant]
While the BA.5 lineage continues to be mainstream in the world, its proportion has been decreasing slightly, and other sublineages and recombinants of the Omicron variant with characteristic mutations in the spike protein have been reported worldwide. In particular, the proportions of the XBB lineage (a recombinant of the BJ.1 lineage (a sublineage of the BA.2.10 lineage) and the BM.1.1.1 lineage (a sublineage of the BA.2.75.3 lineage)) and the XBF lineage (a recombinant of the BA.5.2.3 lineage and the CJ.1 lineage (a sublineage of BA.2.75.3 lineage)) has increased relatively. An increase in proportion has been observed for the XBB.1.5 lineage (a sublineage of XBB lineage) in the US and for the XBF lineage in Australia and other countries. According to the World Health Organization (WHO), etc., it has been pointed out that a predominance of the XBB.1.5 lineage among the increasing number of infected people may be attributed to its ability to escape the immune system, but no findings demonstrating an increased severity in patients infected with the XBB.1.5 lineage has been obtained so far. There are also no clear findings on the BN.1.3 lineage, which has been increasing in Japan. It is necessary to continue collecting and analyzing data on overseas situations and findings regarding the characteristics of these new sublineages and recombinants, and to continue monitoring by genome surveillance.
Figures (Number of new infections reported etc.) (PDF)