Jpn. J. Infect. Dis., 55, 126-127, 2002
To see a printable version of the article in the Adobe file format, crick this [PDF] link.
Laboratory and Epidemiology Communications
Fungal Infection in Neutropenic Patients in a Hospital during Construction
Kan Yonemori*, Naoki Takezako, Kazuko Nishimura1, Tomoko Onose, Fumiko Yamanishi, Hisashi Kawahata, Akihiko Kawana, Namiko Mori, Fumiko Kirikae, Katsutoshi Saruta, Teruo Kirikae, Tadatoshi Kuratsuji, Koichiro Kudo, Oichirou Kobori, Yoshio Yazaki and Tetsuyoshi Miwa
International Medical Center of Japan, Toyama 1-23-1, Shinjuku-ku, Tokyo 162-8655 and 1Research Center for Pathogenic Fungi and Microbial Toxicoses, Chiba University, Inohana 1-8-1, Chuo, Chiba 260-8673
Communicated by Hiroshi Yoshikura
(Accepted August 16, 2002)
Deep fungal infections, caused by Candida, Aspergillus, and other fungi commonly present in the environment (1), are serious problems in immunocompromised hosts, such as in patients with bone marrow transplants and in those with prolonged neutropenia due to intensive immunosuppressive chemotherapy (2). We report here an outbreak of such fungal infections associated with the reconstruction of a building in a hospital.
A building was demolished and then a new building was constructed in its place in a hospital with 925 beds. Demolition and excavation took place from September 2000 to April 2001, and building construction proceeded from March 2002 to the present day. The demolished building faced the north side of the wards of another building.
Four patients (P1, P2, P3, and P4) were hospitalized for treatment of acute myeloblastic leukemia in the hematology ward on the 5th floor of the undemolished building. The patients (mean age, 67 years old; three males and one female) had prolonged neutropenia (<500/mm3) due to chemotherapy. Three patients (P1, P2, and P3) developed high fever, cough with sputum, and dyspnea on October 19, 26, and 27, 2000, respectively. Another patient (P4) had similar symptoms on December 10. The chest x-ray and CT scan of all four patients showed nodular lesions and consolidation in the lobes of the lungs. Cultures and microscopic examination of sputum, urine, and blood were negative for pathogenic bacteria and fungi. However, serum levels of a fungal-specific cell-wall component, (1ü©3)-b-D glycan, as detected by a Fangitech GTM test (Seikagaku Co., Tokyo), were 20 - 40 pg/ml (10 - 20 fold higher than normal levels at <2 pg/ml) in all of the four patients. Antibacterial chemotherapy with broad-spectrum antibiotics was ineffective. Biopsy using a bronchial endoscope was not performed due to the high risk of bleeding. The patients were diagnosed as having "probable invasive fungal infection" by diagnostic criteria of the European Organization for Research and Treatment of Cancer (EORTC) guidelines (3), and they were treated with antifungal antibiotics, amphotericin B (5 - 20 mg/body/day), or itraconazole (200 mg/body/day). Two to three days after treatment, the clinical symptoms improved. One to two weeks after treatment, no symptoms due to infection were observed, and serum levels of (1ü©3)-b-D glycan declined to 50% of the pretreatment levels; moreover, the abnormal findings on the chest x-rays had improved.
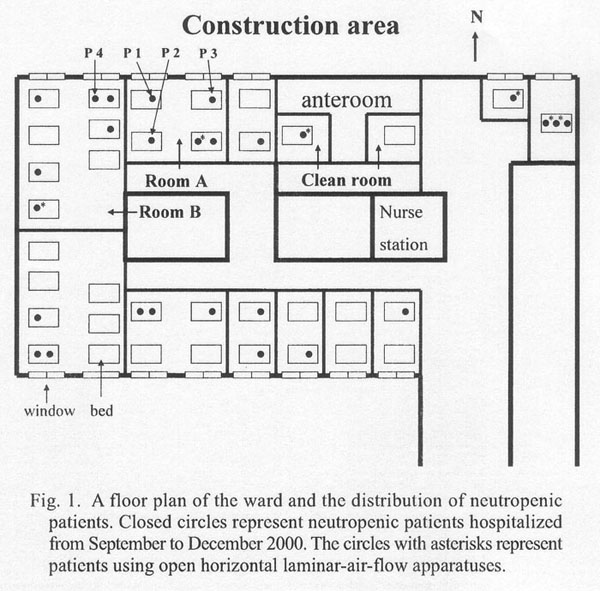
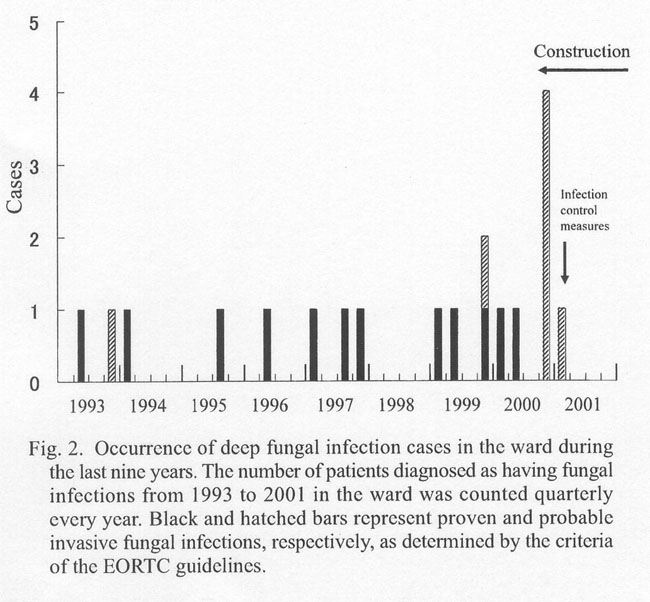
Figure 1 shows a floor plan of the ward and the locations of the room of the four leukemia patients, P1 - P4. The ward had many other neutropenic patients, there was at least one such patient in each room. However, the patients with deep fungal infections stayed in the two rooms facing the construction area (Fig. 1). Patients P1, P2, and P3 were in room A, and P4 was in the adjacent room B (Fig. 1). These rooms were not positive-pressure rooms, and the windows were frequently left open. Figure 2 shows a number of patients in the same ward diagnosed as having "proven or probable invasive fungal infection" (EORTC guidelines) at various periods from 1993 to 2001. At the peak of deep fungal infection cases in the fourth quarter of 2000, the collective cases assumed the features of an outbreak.
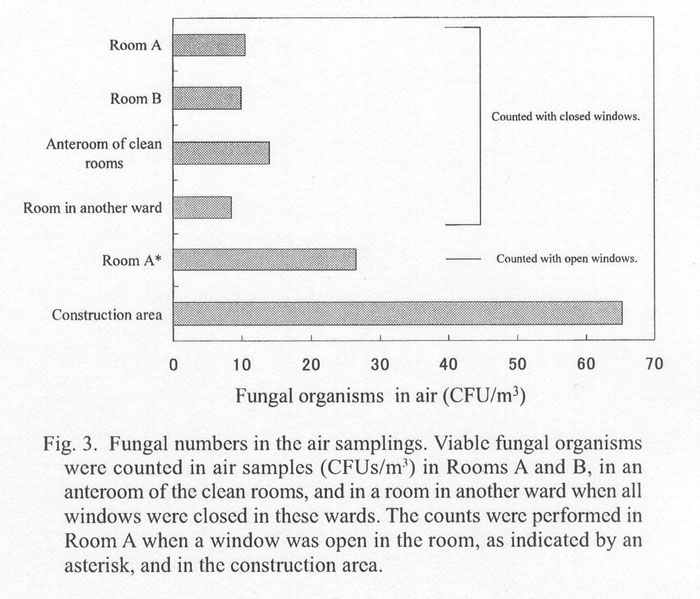
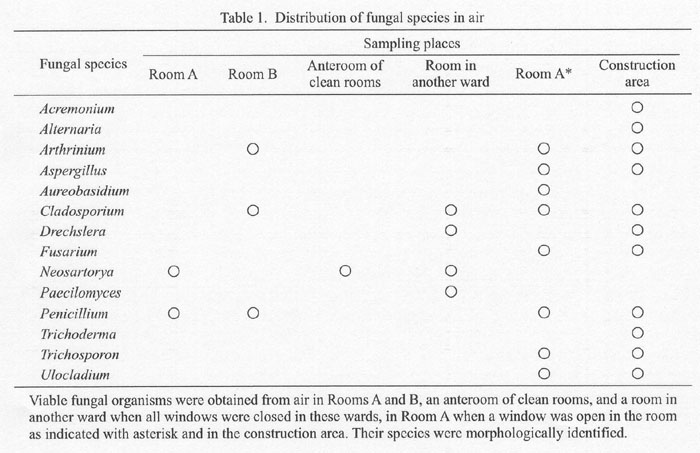
To investigate whether the construction was associated with the fungal infection outbreak in the ward, environmental sampling was performed using a microbiologic air sampler (100 l/min x 10 min, impactor-type on solid surfaces, BIO SAMP MBS-1, Midori-Anzen Co., Tokyo) with Sabroud agar plates to culture the fungal spores. The sample plates were incubated at 35üÄ for 2 to 5 days, and fungal colonies were counted and their species were morphologically determined. Detection of fungi was 10 CFU/m3 in rooms A, B, and in other rooms when all windows in the wards were closed (Fig. 3). In room A, when the windows were kept open, the presence of fungi was about 2.5 times higher than when the windows were closed. About 65 CFU/m3 of fungi were counted in the construction area. As regards the fungal species, one to four species were detected in rooms A and B, in the anteroom of the clean rooms, and in a room in another ward. Eight species were detected in room A when the windows were open and 11 species were in the construction area; seven species were common to both (Table 1). The demolition of the building most likely caused a dispersion of fungi, which reached the nearby ward.
The following measures were taken in the affected ward starting in March 2001: i) all windows were sealed, ii) portable open horizontal laminar-air-flow apparatuses were placed at the bedsides of the neutropenic patients, and iii) itraconazole was prophylactically administered to all neutropenic patients. Thereafter, no fungal infections occurred in the ward.
REFERENCES
*Corresponding author: Fax: +81-3-3207-1038, E-mail: kyonemor@ncc.go.jp
Go to JJID Homepage Go to JJID Contents 55 (4)
{kind=link}
{kind=link}
{kind=link}
{kind=link}