Jpn. J. Infect. Dis., 55, 213-214, 2002
To see a printable version of the article in the Adobe file format, click this [PDF] link.
Laboratory and Epidemiology Communications
Pulmonary Mycobacterium avium Infection in an Immunocompetent Aged Woman Related to Use of Home Bath with a Circulating Water System
Makoto Takahara*, Toshiro Kano, Michiyo Aiyoshi, Tomoko Fujino1, Yayoi Otsuka1, Katsutoshi Saruta1, Tadatoshi Kuratsuji1 and Teruo Kirikae1
National Nishi-Kofu Hospital, Yamamiya 3368, Kofu-shi, Yamanashi 400-0075 and 1International Medical Center of Japan, Toyama 1-21-1, Shinjuku-ku, Tokyo 162-8655
Communicated by Hiroshi Yoshikura
(Accepted February 3, 2003)
Unsuitable management of bath water occasionally causes waterborne infectious diseases, such as infections due to non-tuberculosis mycobacteria (1-3).
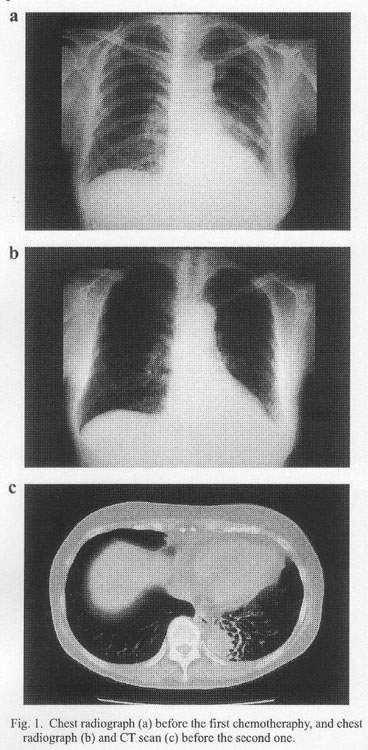
A 65-year-old female consulted her home doctor in regard to a productive cough and general fatigue. She was a non-smoker. She had hypertension and hyperlipidemia. She ran an electrical instrument store with her husband. Her sputum was positive for acid-fast bacilli (AFB) in culture. It was not bacteriologically confirmed at that time whether the bacilli were Mycobacterium tuberculosis or non-tuberculosis mycobacteria. She was referred to the National Nishi-Kofu Hospital for treatment of pulmonary tuberculosis in October 1999. A chest radiograph revealed an infiltration shadow in the lower part of the left lung (Fig. 1a). Sputum examinations were repeatedly negative for both AFB smear and culture. She was treated as an outpatient with combination of isoniazid, rifampin, and ethambutol for 6 months, and with isoniazid and rifampin for the following 3 months. After 9 months of treatment, her symptoms improved and abnormalities in the chest radiograph disappeared.
She had a relapse in September 2001 and visited the National Nishi-Kofu Hospital again. A chest radiograph revealed an increasing shadow in the left costophrenic angle (Fig. 1b), where bronchiectatic lesions were found by CT scan (Fig. 1c). Her sputum was positive for AFB smear and M. avium complex (MAC) culture. Polymerase chain reaction (PCR) (COBAS AMPLICORTM MTB, M. avium and M. intracellulare tests: Roche Diagnostics, Branchburg, N.J., USA) detected M. avium but no M. tuberculosis nor M. intracellulare. Three-drug chemotherapy consisting of clarithromycin, rifampin, and ethambutol was started immediately. The sputa remained positive for MAC in culture and for M. avium in PCR for at least 3 months after start of the treatment. Both culture and PCR then became negative and, after 15 months of treatment, her symptoms and chest radiograph improved.
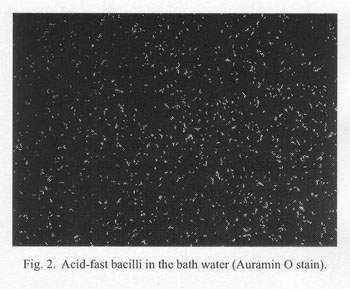
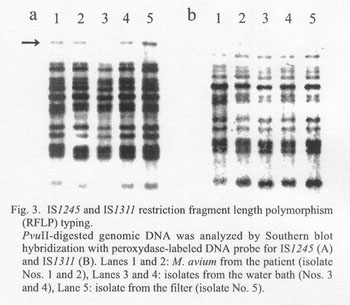
The patient and her husband used a bath with a circulating and filtering water system in their home. Her husband was healthy. His sputum was AFB culture-negative and his chest radiograph showed no abnormality. The bath water and the filter pellets used in the water system were found AFB smear-positive (Fig. 2) and MAC culture-positive. PCR-based diagnosis revealed that the MACs from the bath water and from the filter were both M. avium. To determine whether these isolates and those from the patient were of the same origin, chromosomal DNAs from two isolates derived from the patient, two from the water, and one from the filter were analyzed by IS1245 restriction fragment length polymorphism (RFLP) typing (4) (Fig. 3a) and IS1311 RFLP typing (5) (Fig. 3b).
The IS1245 patterns of two isolates derived from the patient's lung specimen (Nos. 1 and 2), those of the bath water-derived specimen (Nos. 3 and 4), and that of the filter pellets-derived specimen (No. 5) were identical except for one band (indicated by an arrow in Fig. 3a). The IS1311 patterns were identical for all the isolates (Fig. 3b). The data indicated that the M. avium isolates from the patient and those from the bath water and the filter were of the same origin. The patient probably acquired the M. avium infection from the bath water. It remains unknown why only the patient, but not her husband, contracted the disease. Though two young women's cases of pulmonary M. avium infection related to circulating home water baths have been reported (2,3), there has been no previous report on aged cases in Japan. As the majority of patients with pulmonary MAC infection are aged women (1), closer investigation of such cases may lead us to a particular environment, such as the circulating water bath.
REFERENCES
*Corresponding author: Fax: +81-55-251-5882, E-mail: takahara@wkoufu.hosp.go.jp
Go to JJID Homepage Go to JJID Contents 55 (6)
{kind=link}
{kind=link}
{kind=link}