Jpn. J. Infect. Dis., 219-221, 2003
To see a printable version of the article in the Adobe file format, click this [PDF] link.
Laboratory and Epidemiology Communications
A Clonal Expansion of Methicillin-Resistant Staphylococcus aureus (MRSA) in a Tuberculosis Ward
Masayoshi Hosoda, Junji Toyama, Kayo Hasada, Tomoko Fujino1, Ryuji Ohtsuki1 and Teruo Kirikae1*
Aichi Prefectural Owari Hospital, Ichinomiya, Aichi 491-0934 and 1International Medical Center of Japan, Toyama 1-21-1, Shinjuku-ku, Tokyo 162-8655
Communicated by Hiroshi Yoshikura
(Accepted February 6, 2003)
Methicillin-resistant Staphylococcus aureus (MRSA) is one of the most important nosocomial pathogens, which are spread primarily by direct or indirect person-to-person contact. Genome typing using pulsed-field gel electrophoresis (PFGE) is a powerful tool for investigating the source, transmission, and spread of MRSA (1).
In August 2001, an MRSA outbreak occurred in a tuberculosis ward in a 350-bed hospital in the Chubu District. The tuberculosis ward had 50 beds with 32 regular medical staff members, including three doctors, 20 nurses, and two assistant nurses. Microbiologists in the hospital's Laboratory Department noticed that bacteria except for Mycobacterium spp., suspected of MRSA, were frequently isolated in sputum samples from tuberculosis patients, even when the samples were decontaminated for 15 min with the same volume of a 1:1 mixture of 4% sodium hydroxide and 2.9% sodium citrate supplemented with 12 mg/ml of N-acetyl L-cysteine prior to mycobacterial culture. After MRSA surveillance, 17 MRSA isolates were obtained from 15 inpatients.
These 17 isolates and four MRSA isolates obtained in other wards at the same time were tested for chromosomal DNA typing by using a contour-clamped homogeneous electric field system (CHEF MapperTM, Bio-Rad Laboratories, Hercules, Calif., USA), antibiotic susceptibility (WalkAwayTM, Dade Behring, Deerfield, Ill., USA), enterotoxin serotyping (SET-RPLA, Denka Seiken Co., Tokyo), toxic shock syndrome toxin-1 (TSST-1) production (TST-RPLA, Denka Seiken), and coagulase serotyping (Denka Seiken).
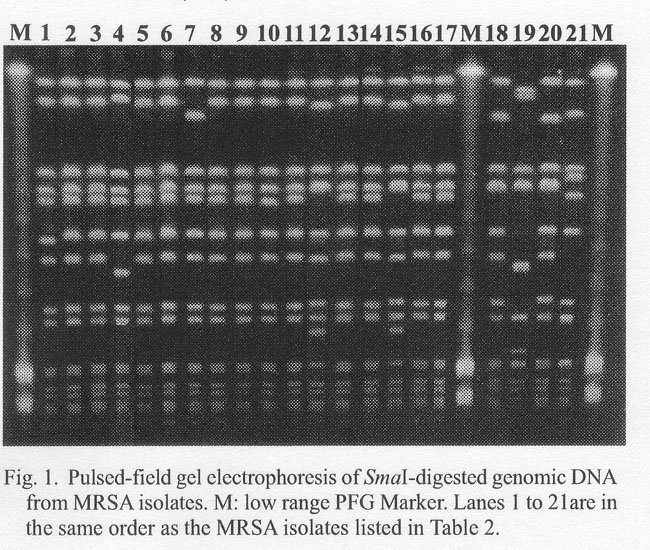
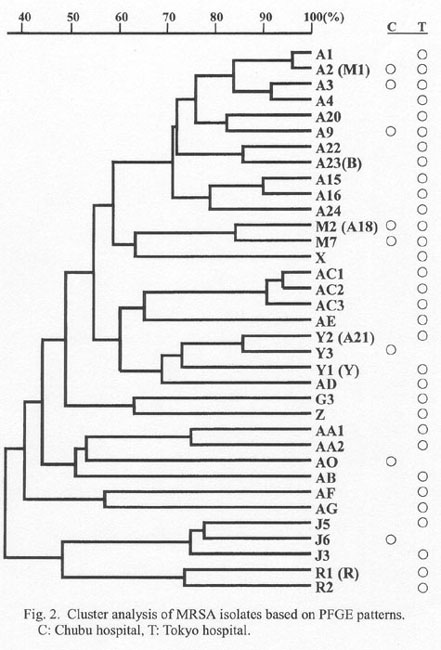
PFGE patterns of the SmaI DNA digests of the 21 isolates are shown in Fig. 1. Figure 2 shows the results of cluster band-based analysis of PFGE patterns (Molecular AnalystTM, Bio-Rad) of these isolates together with all the MRSA isolates obtained from a hospital in Tokyo in October 2002 (1). Isolates from this hospital consisted of eight PFGE patterns; A2, A3, A9, M2, M7, Y3, AO, and J6. Isolates from the hospital in Tokyo consisted of 32 PFGE patterns, which included all the patterns found in the hospital in the Chubu District, except for Y3, AO, and J6. In Fig. 2, we recognize 16 clusters, if patterns with more than a 70% similarity are postulated to form a cluster. In the hospital in Chubu, there were five clusters. In the hospital in Tokyo there were four clusters among the five detected in the hospital in Tokyo. These data indicate the clonal expansion of MRSA not only within hospitals but also nationwide.
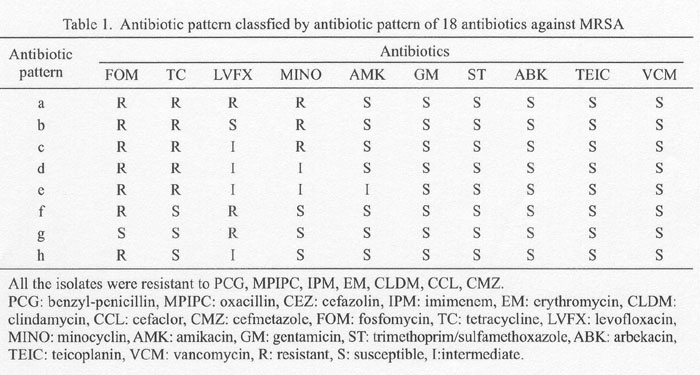
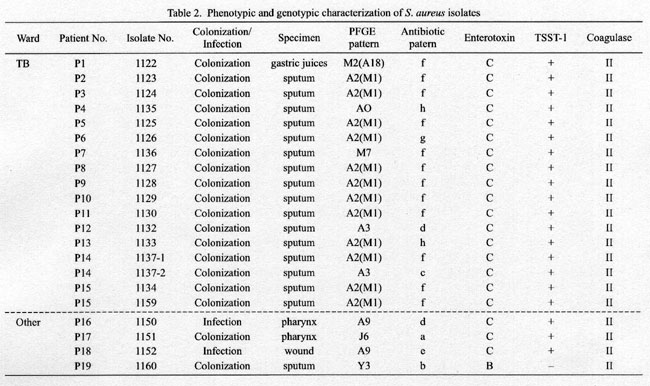
Eight different antibiotic sensitivity patterns, a to h, were seen among Chubu isolates (Tables 1 and 2). Nineteen Chubu isolates produced enterotoxin type C, TSST-1, and coagulase type II (Table 2), while one strain (No. 1160) produced enterotoxin B and coagulase type II, but not produce TSST-1.
It was remarkable that 10 isolates from 11 inpatients in the tuberculosis ward (Nos. 1123, 1124, 1125, 1127, 1128, 1129, 1130, 1137-1, 1134, and 1159) had the same character, i.e., enterotoxin type C, TSST-1 positive, coagulase type II, the same PFGE patterns of SmaI DNA digests, A2(M1), and the same spectrum of antibiotic susceptibility, pattern f. Two other isolates, Nos. 1126 and 1133, had almost identical characters except for a minor difference in antibiotic susceptibility (Tables 1 and 2). Two other isolates from the tuberculosis ward (Nos. 1132 and 1137-2) had the same PFGE pattern, A3. Four isolates obtained from other wards at the same period had PFGE patterns and antibiotics resistance patterns different from those from the tuberculosis ward (Table 2). These results indicate that clonal expansion of MRSA occurred within the tuberculosis ward.
The main mode of transmission of MRSA is via hands, which may become contaminated by direct or indirect contact with colonized or infected persons. Most patients in a tuberculosis ward could exercise a higher level of daily activity as compared to other patients, and had a greater chance of direct or indirect contact with each other. This could have brought about the MRSA outbreak in the tuberculosis ward as in another case reported previously (2). Infection control measures against contact transmission as well as air-borne infection, including education to inpatients, are necessary in tuberculosis wards.
REFERENCES
*Corresponding author: Fax: +81-3-3202-7181, E-mail: tkirikae@ri.imcj.go.jp
Go to JJID Homepage Go to JJID Contents 55 (6)
{kind=link}
{kind=link}
{kind=link}
{kind=link}