Jpn. J. Infect. Dis., 56, 127-129, 2003
To see a printable version of the article in the Adobe file format, click this [PDF] link.
Laboratory and Epidemiology Communications
Clinical Study of Pediatric Cases of Acute Respiratory Diseases Associated with Human Metapneumovirus in Japan
Shinichi Takao*, Hiroyuki Shimozono1, Hiroshi Kashiwa1, Yukie Shimazu, Shinji Fukuda, Masaru Kuwayama and Kazuo Miyazaki
Division of Microbiology II, Hiroshima Prefectural Institute of Health and Environment, Hiroshima 734-0007 and 1Department of Pediatrics, Mazda Hospital, Mazda Motor Corporation, Hiroshima 735-8585
Communicated by Hiroo Inouye
(Accepted July 14, 2003)
*Corresponding author: Division of Microbiology II, Hiroshima Prefectural Institute of Health and Environment, Minami-machi 1-6-29, Minami-ku, Hiroshima 734-0007, Japan. Fax: +81-82-252-8642, E-mail: takao@urban.ne.jp
In 2001, van den Hoogen et al. in the Netherlands initially isolated a new paramyxovirus from a child with acute respiratory tract infections, and termed it human metapneumovirus (hMPV) (1). Later, hMPV was detected in patients with acute respiratory infectious diseases in many countries such as Australia (2), Canada (3), United Kingdom (4), and France (5). In Japan, Goto et al. isolated hMPV from a child with influenza-like illness, clarifying the presence of hMPV infectious disease in Japan (6). However, many points remain to be resolved regarding its clinical and epidemiological states. Here, we summarize the clinical findings of seven pediatric patients whose hMPV infection was confirmed by hMPV-specific RT-PCR.
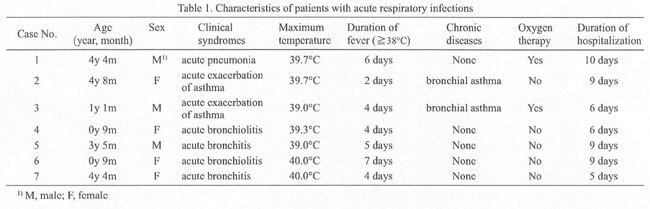
Among patients with acute respiratory tract diseases hospitalized at Mazda Hospital in April 2003, hMPV infection was confirmed by virological examinations in seven patients. Their characteristics are shown in Table 1. The patients were children of 9 months to 4 years 8 months of age (mean: 2 years 9 months). The clinical symptoms were acute exacerbation of bronchial asthma in two patients, acute bronchiolitis in two patients, acute bronchitis in two patients, and acute pneumonia with hypoxia in one patient. No patient had underlying disease of the central nervous system, respiratory system, or renal system. Two cases (Cases 2 and 3) had bronchial asthma. All patients developed fever of 39ĪC or higher at its peak and the fever persisted for 2 to 7 days (mean: 4.6 days). The duration of hospitalization ranged from 5 to 10 days (mean: 7.7 days). Case 1 and Case 3 required oxygen inhalation therapy for hypoxia due to pneumonia and asthmatic attack, respectively. However, both patients had recovered well and were discharged without any sequela.
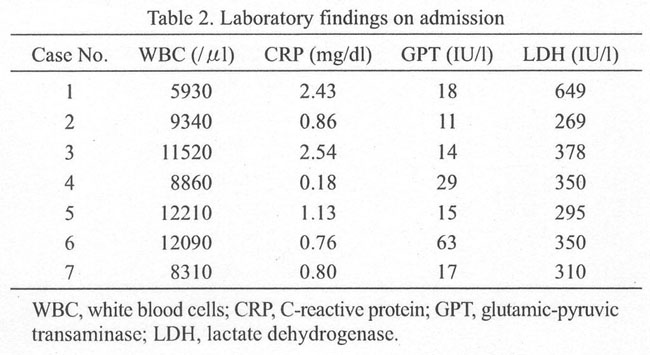
The laboratory findings in the patients on admission are shown in Table 2. Their white blood cell count was 5,930-12,210/ml (mean: 9,751/ml) and CRP was 0.18-2.54 mg/dl (mean: 1.24 mg/dl), showing no leukocytosis, leukopenia, or increased CRP. GPT was slightly increased in one patient (Case 6), but was within the normal range in the other six patients.
The findings of the virological examinations performed using nasopharyngeal aspirates and sera collected at admission are shown in Table 3. Viral tests using commercial rapid diagnosis kits showed all patients negative for adenovirus antigen and influenza virus A and B antigens. One patient (Case 1) was positive for respiratory syncytial virus (RSV) antigen, but the other six patients were negative. All six patients examined were negative for serum IgM antibody against Mycoplasma pneumoniae. On virus isolation, which we routinely perform using six types of cultured cells including MDCK cells, no respiratory viruses such as influenza virus, rhinovirus, parainfluenza virus, adenovirus, enterovirus, or herpes simplex virus were isolated. Viral RNA extracted from nasopharyngeal aspirates was subjected to nested RT-PCR using primers (MPVF1f:5'-CTTTGGACTTAATGACAGATG-3', MPVF1rüF5'-GTCTTCCTGTGCTAACTTTG-3') that amplify a 450-bp fragment in the region encoding hMPV fusion protein reported by Peret et al. (7), and primers (MPVF2f:5'-CATGCCGACCTCTGCAGGAC-3', MPVF2r: 5'-ATGTTGCAYTCYYTTGATTG-3') designed by us that amplify a 357-bp fragment targeting at a further inner region of the above. The gene specific to hMPV was amplified in all seven patients. The nucleotide sequence was determined in order to confirm the identity of the virus detected by the RT-PCR reaction. As a result, the nucleotide sequences of the amplicons (Gene Bank accession no.: AB113371 to AB113374) had 95% to 97% homology with the previously described F gene sequences in GenBank.
Mazda Hospital is located in a region with a large young urban population, and adenoviral infections and mycoplasmal pneumonia occur throughout the year, although the number of patients varies seasonally. Since several patients with lower respiratory tract infections negative for adenovirus antigen or anti-Mycoplasma IgM antibody were observed at Mazda Hospital in April 2003 when an influenza epidemic subsided, the hMPV test was performed in these patients, and seven patients were hMPV-positive. They had relatively severe respiratory symptoms such as persistent high fever, productive cough, and dyspnea. Freymuth et al. examined the clinical syndromes in 26 children admitted for acute respiratory infectious diseases; 16 patients had acute bronchiolitis, four patients had acute exacerbation of bronchial asthma, and the other patients had acute bronchitis, laryngitis, and high fever (5). Two of our seven patients also had acute exacerbation of bronchial asthma. Infection with rhinovirus, influenza virus, RSV, and M. pneumoniae is known to induce acute exacerbation of bronchial asthma. hMPV may be another causative agent for aggravating asthma symptoms. Among the seven patients, the 4-year-old patient (Case 1) showed the severest symptoms with prolonged high fever and tachypnea suggesting viral pneumonia, though he did not have any particular underlying disease and had been healthy. This patient needed hospitalization for high fever and tachypnea. On chest X-ray examination on admission, infiltration and rough large cord-like shadows were noted mainly in the hilar regions of the bilateral lung fields (Fig. 1). He developed respiratory distress and his arterial oxygen saturation was low (89-90%), indicating hypoxia. The patient was immediately placed in an oxygen tent after admission. The oxygen concentration was adjusted to 40%, and 2 mg/kg/day predonisolone was administered intravenously, after which dyspnea and high fever had resolved. This patient had superinfection of hMPV and RS virus. Greensill et al. suggested that superinfection of RSV and hMPV may aggravate respiratory symptoms of bronchiolitis (8). Superinfection with the two viruses may have caused the respiratory distress observed in Case 1 with pneumonia.
From March to June of 2003, hMPV was detected from pediatric patients with acute respiratory infections in various parts of Hiroshima Prefecture. It may indicate a seasonal prevalence of hMPV infections in Japan as in other countries. Analysis of virological and clinical data obtained from the hMPV-infected children is now in progress.
REFERENCES
Go to JJID Homepage Go to JJID 56 (3) Contents
{kind=link}
{kind=link}
{kind=link}
{kind=link}