Jpn. J. Infect. Dis., 56, 132-133, 2003
To see a printable version of the article in the Adobe file format, click this [PDF] link.
Laboratory and Epidemiology Communications
Molecular Epidemiology of Intra-Familial Tuberculosis Transmission
Makoto Takahara*, Yoshiharu Yajima, Sumio Miyazaki, Michiyo Aiyoshi, Tomoko Fujino1, Yayoi Otsuka1, Jun-ichiro Sekiguchi1, Katsutoshi Saruta1, Tadatoshi Kuratsuji1 and Teruo Kirikae1
National Nishi-Kofu Hospital, Yamanashi 400-0075 and 1International Medical Center of Japan, Tokyo 162-8655
Communicated by Hiroshi Yoshikura
(Accepted July 22, 2003)
*Corresponding author: Mailing address: National Nishi-Kofu Hospital, Yamamiya 3368, Kofu-shi, Yamanashi 400-0075, Japan. Fax: +81-55-251-5882, E-mail: takahara@wkoufu.hosp.go.jp
The risk of tuberculosis transmission has been estimated to be relatively high among household contacts of index tuberculosis patients (1). We report here two cases of tuberculosis transmission from index patients to family members, based on restriction fragment length polymorphism (RFLP)-analysis of the pathogens.
Case 1: A 43-year-old male (patient A1) visited his home doctor complaining of fever and a left chest pain. He had smoked 15 cigarettes per day for 27 years. At the age of 28, he had experienced right side pneumothorax. He worked in a factory. He was single and lived with his father and sister. A chest radiograph revealed a cavitary lesion in the left apical region and left pleural effusion. A CT scan confirmed the cavitary lesion. He was referred to a city hospital in Yamanashi Prefecture. His sputum was negative for acid-fast bacilli (AFB). His bronchial lavage was positive for both AFB and Mycobacterium tuberculosis cultures. His gastric juice was positive for M. tuberculosis in polymerase chain reaction (PCR) (COBAS AMPLICORTM MTB, Roche Diagnostics, Branchburg, N.J., USA). He was referred to a national hospital for treatment of pulmonary tuberculosis. The household contact investigation then performed revealed that his father (patient A2), but not his sister, had contracted tuberculosis. His father had no symptoms. He was a 73-year-old retired man, who had smoked 30 cigarettes per day for 50 years. He had hypertension. His sputum was positive for AFB and M. tuberculosis culture. A chest radiograph showed multiple small cavitary lesions in the bilateral upper lung fields. His chest CT scan revealed centrilobular infiltrations in the right upper lung field.]
Case 2: A 54-year-old male (patient B1) visited his home doctor in October 2001 with complaints of fatigue, fever, shortness of breath, and a 20 kg loss of body weight over the previous 3 months. He had smoked 20 cigarettes per day for 37 years and was a carpenter. His father had died of tuberculosis after being ill for 10 years. His sputum was positive for AFB and M. tuberculosis-positive in culture and PCR. His chest radiograph revealed multiple cavitary lesions in the bilateral upper and middle lung fields. He was referred to the national hospital for treatment of pulmonary tuberculosis in October 2001. His son (patient B2), a 25-year-old office worker who lived with him until 2000, was referred to the same hospital in February 2002 when a routine radiograph check revealed an abnormal shadow. He had smoked 20 cigarettes per day for 6 years. His sputum was positive for AFB and M. tuberculosis-positive in culture and PCR. A chest radiograph revealed a cavitary lesion in the left upper field and infiltration shadows in the left middle and right upper lung fields. His chest CT scan showed a cavitary lesion in the left apical region. He was admitted for treatment of pulmonary tuberculosis.
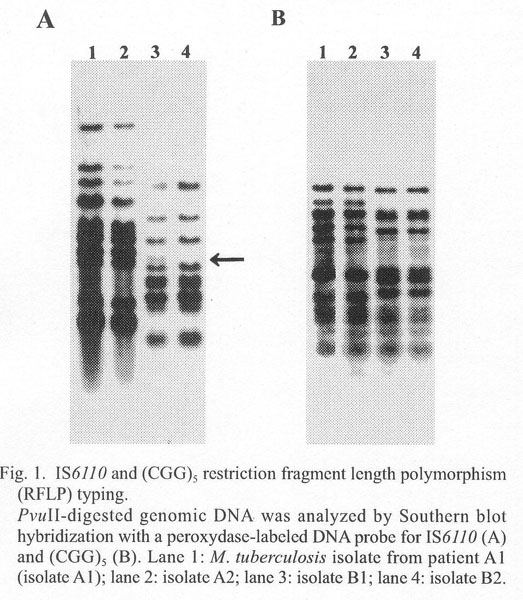
To determine whether the strains of M. tuberculosis infecting the respective patients and their contacts were of the same origin, chromosomal DNAs from these isolates were analyzed by RFLP using a IS6110 probe (4) (Fig. 1A) and a trinucleotide repeat sequence (CGG)5 probe (Y. Otsuka et al., in preparation for a paper) (Fig. 1B).Å@The IS6110 patterns were identical for isolates from patients A1 and A2 (lanes 1 and 2). The IS6110 patterns of isolates from patients B1 and B2 were identical except in one band (indicated by an arrow in Fig. 1A), and differed from the pattern observed in isolates A1 and A2. The (CGG)5 pattern was identical between isolates A1 and A2, and between isolates B1 and B2, respectively. All these isolates were sensitive to isoniazid, rifampin, pyrazinamide, ethambutol, and streptomycin. No mutations were found in the drug resistance-related genes, including katG and inhA responsive for isoniazid-resistance, rpoB for rifampin-resistance, pncA for pyrazinamide, embB for ethambutol-resistance, rrsL and rrs for streptomycin, and gyrA for flouroquinolones. The data indicated that M. tuberculosis isolates A1 and A2, and isolates B1 and B2, respectively, were of the same origin. The data clearly supported transmission of M. tuberculosis within a family.
The authors thank Dr. F. Ikeda, Nirasaki City Hospital, for critical comments on Case 1. Patients A2 and B2 requested the epidemiological analysis described herein.
REFERENCES
Go to JJID Homepage Go to JJID 56 (3) Contents
{kind=link}