Jpn. J. Infect. Dis., 56, 175-177, 2003
To see a printable version of the article in the Adobe file format, click this [PDF] link.
Laboratory and Epidemiology Communications
Vaccination Coverage of Poliomyelitis among Less than 5-Year-Old Children in the Markets of Niger
Midori Kobayashi, Keiko Hirakawa, Michihisa Sawada, Chiemi Suzuki, Syuhei Saikawa, Hiroko Ando, Miyuki Nakane1 and Takashi Nakano 2*
Niger Polio Control Team, Japan Overseas Cooperation Volunteers, Japan International Cooperation Agency, Tokyo 151-8558, 1Agency for Cooperation in International Health, Kumamoto 862-0901 and 2Department of International Health and Pediatrics, Institute for Clinical Research, National Mie Hospital, Mie 514-0125
Communicated by Hiroshi Yoshikura
(Accepted August 11, 2003)
* Corresponding author: Mailing address: Department of International Health and Pediatrics, Institute for Clinical Research, National Mie Hospital, Ozato-Kubota 357, Tsu, Mie 514-0125, Japan. Fax: +81-59-232-5994, E-mail: nakano@mie-m.hosp.go.jp
As part of its contribution to the global polio eradication program, the Japan International Cooperation Agency (JICA) is sending a Polio Control Team of Japan Overseas Cooperation Volunteers (JOCV) to Niger since 1999. Its field of activity is Maradi Prefecture, having a 280 km international border with Nigeria. As the latest polio cases have been reported only from the Niger/Nigeria border region, Maradi is considered a high risk area (1). The main activities of polio control team are promoting "surveillance on acute flaccid paralysis (AFP)" and supporting "national immunization days (NIDs) of oral polio vaccine (OPV)".
Niger implemented NIDs since 1997 as one of the strategies of polio eradication. The wild poliovirus continued to be isolated (3 cases in 2000; 6 in 2001; 3 in 2002) in spite of repeated NIDs and its reported coverage of more than 90% of the country (2). However, as wild type poliovirus isolation is usually accompanied with low vaccination coverage, non-vaccinated groups remain. Identifying such groups and making OPV available to them is of prime importance.
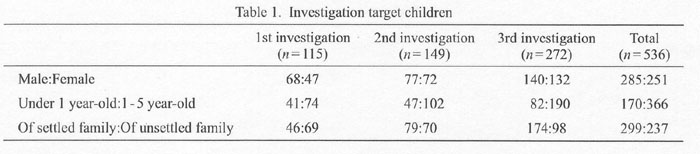
In four markets in Dakoro County of Maradi, JOCV and the Niger Red Cross, Dakoro County Branch, conducted a joint questionnaire-based survey of mothers with children under the age of 5 years. In the three surveys conducted from 27 April - 9 May 2001, from 21 - 24 August 2001, and from 5 - 8 March 2002, a total of 536 mothers were interviewed: 115 mothers in the first, 149 in the second, and 272 in the third survey. The children of the 536 interviewed mothers were 285 boys and 251 girls, 170 under 1 year-old, and 366 aged 1 - 5 years. Two hundred and ninety-nine children were from settled families and 237 were from unsettled families including nomads (Table 1).
They were asked about OPV history (NIDs or routine vaccination) and their awareness of OPV or the reason he/she had not been vaccinated. BCG scars were checked also. In analysis of NIDs coverage, the children born after the latest NIDs were excluded.
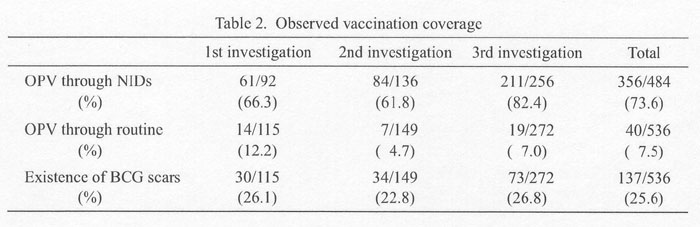
The portion of surveyed children who had OPV through NIDs were around 60% in the first and the second surveys, but increased to 82.4% in the last survey. If the results of the three surveys were totaled, such children were 73.6% (356/484). The portion of children who had OPV through routine vaccination was only 7.5% (40/536). Malfunction of routine vaccination has also been reported in China (3). BCG coverage, another routine vaccine under Expanded Programme on Immunization (EPI), was 25.6% (137/536)(Table 2). Among 299 children of settled families, those with more than one OPV (NIDs or routine) were 231 (77.3%) and those with BCG scars were 93 (31.1%). Among 237 children of unsettled families, 134 cases (56.5%) had OPV histories and 44 cases (18.6%) BCG scars.
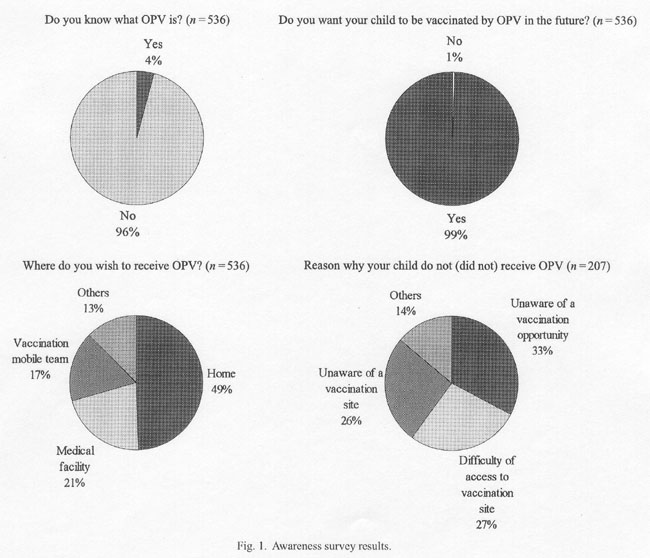
Regarding mothers' awareness of OPV (Fig. 1), only 21 mothers (4%) knew what OPV was. However, 533 mothers (99.4%) wanted their child vaccinated with OPV in the future. As for the place for OPV vaccination, 265 mothers preferred their houses, 113 medical facilities, and 89 via a mobile vaccination team. Among 207 mothers who were asked about their reasons for missing OPV, 68 mothers (33%) were not aware of the vaccination event, 56 (27%) had difficulty in reaching the vaccination site, and 53 (26%) could not locate the vaccination site. Insufficient information to the residents could be a problem.
Although no mother manifested explicit refusal, some suggested the existence of a person opposing vaccinations, such as saying "a woman ought not decide", "household head should decide", or "my child is too young for vaccination". The number of families refusing OPV during a house visit had not declined. In villages, rumors, such as "a polio vaccine is a contraceptive drug", were circulating. We heard people saying "why polio vaccine while doing nothing for more serious diseases?" A nomad said "the hospital is 3 - 5 km away and too far to reach" though they are travelling more than 10 km to the market. It is important to understand why residents refuse or are reluctant to receive vaccinations.
Table 2 shows that the opportunity for OPV greatly depended on NIDs. Some children among the interviewees were vaccinated in Nigeria or in Mali during their movements. Synchronized NIDs are thus said to be effective for unsettled families in West Africa (2). As already mentioned, the coverage in NIDs was highest in the third survey in comparison the first and second surveys. This may indicate that repeated NIDs may increase the children's opportunity for vaccination. However, we know that the children with zero OPV continue to exist while other children are receiving multiple OPVs.
Children in non-settled families had lower rates of OPV histories as well as BCG scars. People in border areas without fixed residences are frequently sources of polio outbreak (4,5) and they need special attention. In the end-stage of the smallpox eradication program, an outbreak continued among nomads moving about in the Ogaden desert in Africa (6). As mothers' preferred vaccination site appears to be their houses, "House to House" vaccination may be a choice. However, "House to House" immunization of nomads with no fixed address is logically impossible. Immunization of the floating population continues to be a problem.
We would like to express our sincere gratitude to the Niger Government which offered their greatest support to the JOCV's activity for polio eradication and related organizations, including the World Health Organization Niger office, the JOCV Niger office, and the JICA.
REFERENCES
Go to JJID Homepage Go to JJID 56 (4) Contents
{kind=link}
{kind=link}
{kind=link}
{kind=link}