Jpn. J. Infect. Dis., 56, 177-178, 2003
To see a printable version of the article in the Adobe file format, click this [PDF] link.
Laboratory and Epidemiology Communications
An Unusual Outbreak of Infusion-Related Bacteremia in a Gastrointestinal Disease Ward
Keizo Torii, Yasunobu Noda1, Yutaka Miyazaki2 and Michio Ohta*
Department of Bacteriology, Graduate School of Medicine, University of Nagoya, Nagoya 466-8550, 1Division of Pulmonology, Department of Internal Medicine, Toyohashi Municipal Hospital, Toyohashi 441-8570 and 2Aichi Prefectual Institute of Public Health, Nagoya 462-8576
Communicated by Yutaka Miyazaki
(Accepted August 29, 2003)
*Corresponding author: Mailing address: Department of Bacteriology, Graduate School of Medicine, University of Nagoya, Tsurumai-cho 65, Showa-ku, Nagoya 466-8550, Japan. Tel: +81-52-744-2106, Fax: +81-52-744-2107, E-mail: mohta@med.nagoya-u.ac.jp
Pseudomonas putida, P. aeruginosa, and Serratia marcescens are Gram-negative bacteria frequently found in hospital environments. P. aeruginosa and S. marcescens have been recognized as important pathogens of nosocomial infection. They cause serious infections, including meningitis, bacteremia, and pneumonia. Many outbreaks due to these organisms have been reported (1,2).
On June 18 and 19, 2000, five patients in the ward of a city hospital developed high fever. On June 17, they had all been administered anticoagulants or diuretics via the central or peripheral vein. On June 20, suspecting iatrogenic infection, the infection control team of the hospital started an investigation including environmental surveillance and interviews with the ward staff members.
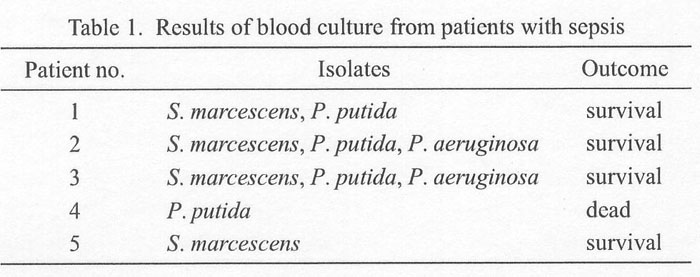
Blood was drawn from the patients for microbiological examination before antibiotic therapy was initiated. From the patients' blood, P. putida, P. aeruginosa, and S. marcescens were isolated (Table 1). Bacterial cultures were also obtained from various sites of the ward, including a basket for placing syringes, the ward's sink, sponges, disinfectant solutions, room surfaces, and staff members' hands. The culture specimens were sent to Aichi Prefectural Institute of Public Health for pulsed-field gel electrophoresis (PFGE). PFGE was performed as described by Nakano and colleagues (3).
Upon identification of pathogens, the patients were immediately moved to an intensive care unit. In the ward, several control measures were implemented. Glass syringes used for preparing intravenous injection fluids (IV fluids) were replaced by disposable plastic syringes. Infected and non-infected areas were strictly separated. Education of the staff in the ward was strengthened, including hand washing before and after each patient contact and cleaning of environmental surfaces with disinfectants.
The team's investigation indicated that the repeated use of glass syringes was the cause of this outbreak. In this hospital, as a convenience, IV fluids were prepared by using glass syringes. Usually, used syringes are washed in the ward's storeroom before returning them to the cleaning unit on every Saturday. In the present outbreak, used syringes were washed on Friday, and returned to the basket. To make matters worse, the basket was returned to the original position without being properly labeled "used". The IV fluids were prepared using these syringes. This could have been a cause of the error.
S. marcescens was isolated from four patients, P. putida from four patients, and P. aeruginosa from two patients (Table 1). All these bacterial species were isolated from the sink.
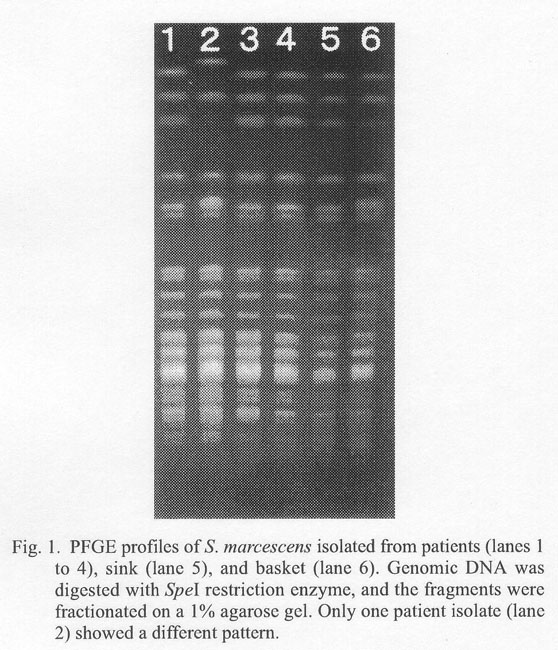
The PFGE patterns of the SpeI-digests of DNA from the six S. marscescens isolates, four from the patients, one from the sink, and one from a basket were identical except for one (Fig. 1). The PFGE patterns of P. putida and P. aeruginosa were almost identical among the patients' isolates, but were totally different between the patients' and environment isolates (data not shown). Therefore, in the present case, the major cause of the outbreak was probably S. marcescens in the environment, which was introduced into IV fluids after repeated use of syringes placed in a contaminated basket. As the PFGE patterns of P. putida and P. aeruginosa were respectively identical among the patient isolates, these two bacteria species probably expanded as clones and came to be involved in the outbreak. Though P. putida is generally considered less virulent than P. aeruginosa, there has been a report that clearly showed an outbreak caused by P. putida (4).
While catheter-related bacteremia is generally caused by Gram-positive bacilli, such as Staphylococcus aureus, coagulase-negative Staphylococcus and Enterococcus, infusate-related bacteremia is often caused by Gram-negative bacteria, such as Klebsiella, Pseudomonas, and Serratia, as in the present case. In most outbreaks, the source of responsible pathogens was difficult to be identified by environmental surveillance, even if the bacteria were isolated from patients (5) or from environment (6). The present investigation fortunately was able to establish the link between the outbreak and the environmental pathogens. As these pathogens cannot be eradicated from the hospital environment, constant infection control measures is needed in order to prevent nosocomial infections.
REFERENCES
Go to JJID Homepage Go to JJID 56 (4) Contents
{kind=link}
{kind=link}