Jpn. J. Infect. Dis., 56, 181-183, 2003
To see a printable version of the article in the Adobe file format, click this [PDF] link.
Laboratory and Epidemiology Communications
Molecular Epidemiology of Type 2 Vaccine-Associated Paralytic Poliomyelitis in China
Yasuo Chiba*, Makoto Kobayashi, Toru Chosa, Teiji Yamamoto1, Kazuhiro Endo1, Hiroyuki Shimizu2, Li Li3, Xu Wen-Bo4 and Zhang Li-Bi4
Bureau of International Cooperation, International Medical Center of Japan, Tokyo 162-8655, 1Department of Neurology, Fukushima Medical School, Fukushima 960-1295, 2Department of Virology ģĀ, National Institute of Infectious Diseases, Tokyo 208-0011, 3Health Economy, University of Tokyo Graduate School of Medicine, Tokyo 113-0033 and 4National Laboratory for Poliomyelitis, Chinese Center for Disease Control and Prevention, Beijing 100050, China
Communicated by Hiroshi Yoshikura
(Accepted September 5, 2003)
*Corresponding author: Mailing address: Bureau of International Cooperation, International Medical Center of Japan, Toyama 1-21-1, Shinjuku-ku, Tokyo 162-8655, Japan.ü@Tel: +81-3-3202-7181, Fax: +81-3-3205-7860, E-mail: ychiba@tkh.att.ne.jp
China's last case of poliomyelitis associated with indigenous wild polioviruses was detected in Fujian Province in 1994. Until 1999, four patients on the China-Myanmar border and one more patients infected by imported wild polioviruses had been reported in China. The virus spread has been contained quickly so far (1). Cases with vaccine-associated paralytic poliomyelitis (VAPP) occur every year in China but the epidemiology of the VAPP remained obscure (2). The occurrence of VAPP is an inevitable but serious problem associated with the use of oral poliovirus vaccine (OPV). After the poliomyelitis outbreaks in Haiti and Dominican Republic in 2000 - 2001, person-to-person transmission of vaccine-derived poliovirus (VDPV) has emerged as a critical issue for achieving global poliomyelitis eradication (3). In order to know the extent of VDPV transmission in China, we conducted nucleotide sequence analysis of type 2 isolates of acute flaccid paralysis (AFP) cases detected in the two southern provinces, Yunnan and Guizhou.
Type 2 Sabin-derived virus has been the main VDPV isolated from AFP in China after the completion of the poliomyelitis free project. The majority of paralytic cases we investigated were indeed due to infections of this serotype (2). We studied VAPP cases in the area covering northeast Yunnan to west Guizhou, which has been known to report more AFP cases than has other parts of China.
Thirteen cases positive for type 2 VDPV occurred in Zhaotong Prefecture, Yunnan Province during 1997 - 2001. Of these, 12 cases were from one county, Zhenxiong. Japanese neurologists made clinical diagnoses of four cases and the local epidemic prevention station investigated the remaining nine cases. Another 13 similar cases occurred in Guizhou Province in the same period. Japanese experts confirmed paralytic polio in all of these cases.
Virus isolation was carried out in provincial polio laboratories. The VDPV isolates were sent to the China National Laboratory for Poliomyelitis for further characterization. For comparion with vaccine viruses, Kunming strain, nucleotide sequence analysis of the whole VP1 region and a part of the 3D region was conducted after intra-typic differentiation by PCR-RFLP.
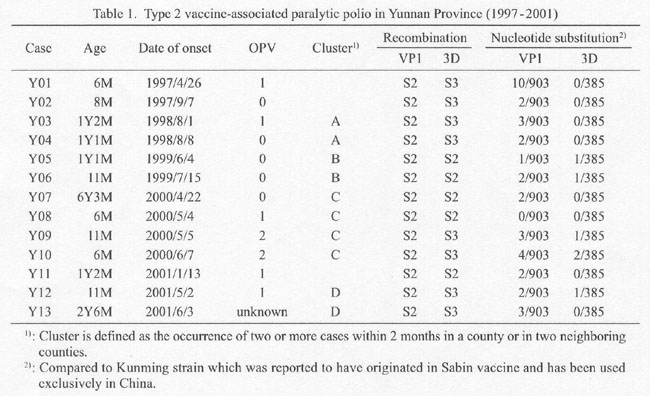
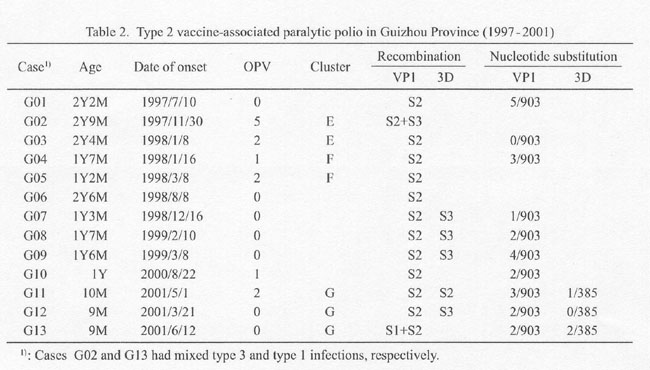
Epidemiologic and virological data of the 26 paralytic cases are presented in Table 1 and Table 2. Of these, 20 patients (76%) were aged less than 2 years. Twenty-four patients (92%) were incompletely immunized with OPV or unvaccinated. No special tendency was seen in the seasonal occurrence of the cases.
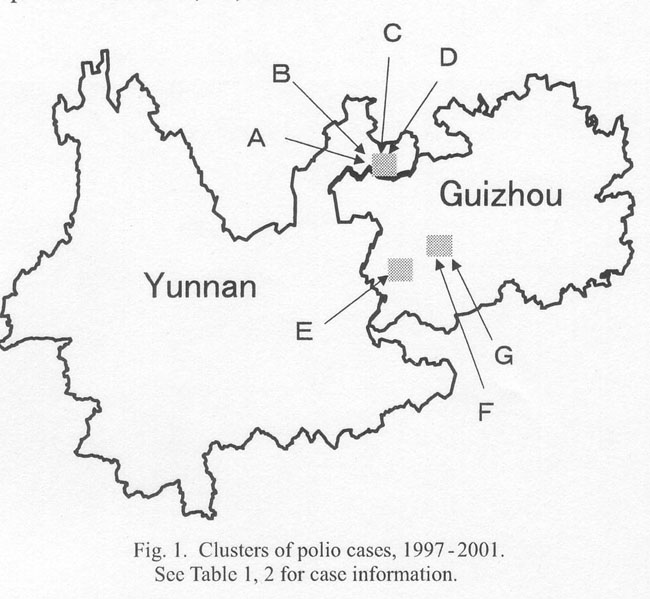
Seven infection clusters, A-G, where two to four cases occurred within 2 months in a same or in two adjacent counties, accounted for 17 cases (Fig. 1). Four of the seven clusters, A-D, were seen in one county, Zhenxiong in Yunnan, while the remaining three clusters, E-G, were in Guizhou.
Among 13 Yunnan isolates including those of the four clusters, eight isolates were recombinants with type 2-derived VP1 and type 3-derived 3D (Table 1). Nucleotide substitution compared to vaccine virus in the VP1 region was less than 1% in the 12 isolates while it slightly exceeded 1% (1.1%, 10/903 nucleotides) in one isolate, YO1. Nucleotide substitution of the 3D region was minimum. Among Guizhou's 13 isolates, four were recombinants with type 2-derived VP1 and type 3-derived 3D (Table 2). Nucleotides substitution of the VP1 region was also less than 1% in these isolates. No genetic relatedness existed among the Yunnan isolates or among Guizhou isolates. These isolates appeared to be independent derivatives of vaccine polioviruses, and were not due to the spread of VDPV with accumulated genomic changes, though they occurred in cluster in time and space.
As the incidence of VAPP in other Chinese provinces, such as Shandong Province, appears to be an acceptable level (2), it is interesting to know why VAPP occurred in clusters so frequently in Yunnan and Guizhou Provinces. This area including southern Sichuan is one of the most inaccessible areas in China and has a relatively high population density, relatively high birth rate, insufficient immunization services, and poor hygienic conditions. Transmission of vaccine viruses to susceptible children in the communities may occur easily in such places though to a limited extent.
In 2000, outbreaks of type 1 VDPV occurred in Haiti and Dominican Republic in the Caribbean Sea. Similar epidemics were reported in Egypt (type 2) and the Philippines (type 1) (4,5). Characterization of such VDPV has been done under international coordination (6). Analysis of the Caribbean type 1 VDPV showed that nucleotide substitution in the VP1 region was 2 - 3% compared to Sabin strain. This is clearly different from nucleotide changes seen in sporadic VAPP cases (<0.5%). Type 2 VDPV suspected of extensive transmission in Egypt during 1988 - 1993 had also greater nucleotides substitution, 4 - 7%, in the VP1 region (4). The nucleotide sequence in the region encoding non-structural proteins was greatly changed in all of the Caribbean isolates and the sequence was shown to have derived from species C non-polio enteroviruses. The VDPV was biologically indistinguishable from wild polioviruses (3), regarding such characteristic as temperature sensitivity and neurovirulence (6).
The viruses implicated in the AFP clusters described in the present report are quite different from these VDPV cases, and close to the original vaccine strains. However, one type 2 isolate in Yunnan in 1997 was shown to have genomic changes suggesting limited circulation in the past, and six type 2 vaccine polioviruses isolated from three poliomyelitis cases and their contacts in southern Sichuan Province in June 2002 were found to be clonal, indicating person-to-person spread (though nucleotide substitution in the VP1 region was three nucleotides at most) (Chinese CDC, unpublished document). Sustaining population immunity at a high level is probably important to minimize VAPP caused by a minimally mutated vaccine virus as in the case of extensively circulating VDPV (3,6).
This study was supported in part by grants-in-aid for "Development of Expanded Programme on Immunization (EPI) and Accelerating Measles Control in the Polio-free Era" from the Ministry of Health, Labour and Welfare, Japan.
References
Go to JJID Homepage Go to JJID 56 (4) Contents
{kind=link}
{kind=link}
{kind=link}