Jpn. J. Infect. Dis., 57, 181-182, 2004
To see a printable version of the article in the Adobe file format, click this [PDF] link.
Laboratory and Epidemiology Communications
A Small Outbreak of Third Generation Cephem-Resistant Citrobacter freundii Infection on a Surgical Ward
Toshi Nada*, Hisashi Baba, Kumiko Kawamura2, Teruko Ohkura, Keizo Torii1 and Michio Ohta1
Department of Clinical Laboratory, Nagoya University Hospital, Nagoya 466-8560, 1Department of Bacteriology, Nagoya University Graduate School of Medicine, Nagoya 466-8550 and 2Department of Medical Technology, Nagoya University School of Health Sciences, Nagoya 461-8673
Communicated by Yoshichika Arakawa
(Accepted June 11, 2004)
*Corresponding author: Mailing address: Department of Clinical Laboratory, Nagoya University Hospital, Tsurumaicho 65, Showa-ku, Nagoya 466-8560, Japan. Tel: +81- 52-744-2614, Fax: +81-52-744-2613, E-mail: t-nada@med.nagoya-u.ac.jp
Citrobacter freundii is a member of family Enterobacteriaceae and has been associated with nosocomial infections in the urinary, respiratory, and biliary tracts of debilitated hospital patients. C. freundii has an inducible chromosomally encoded cephalosporinase that can inactivate cephamycins and cephalosporins. However, most clinical isolates are sensitive to new third generation cephems and carbapenems.
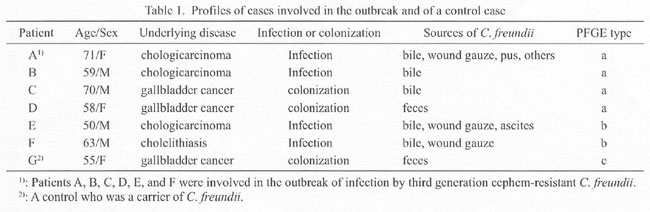
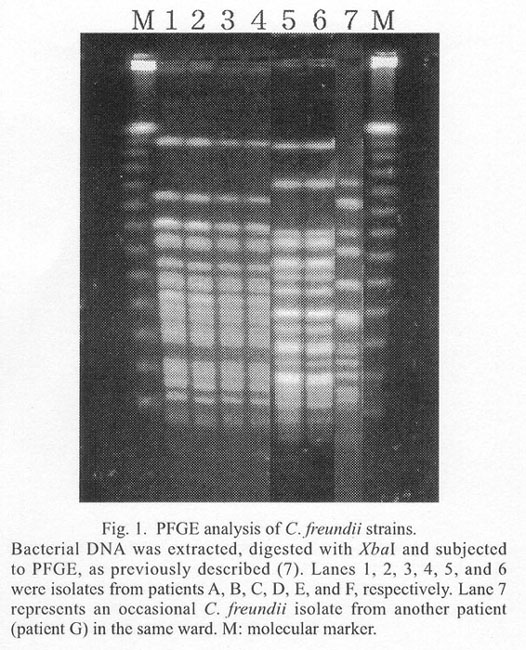
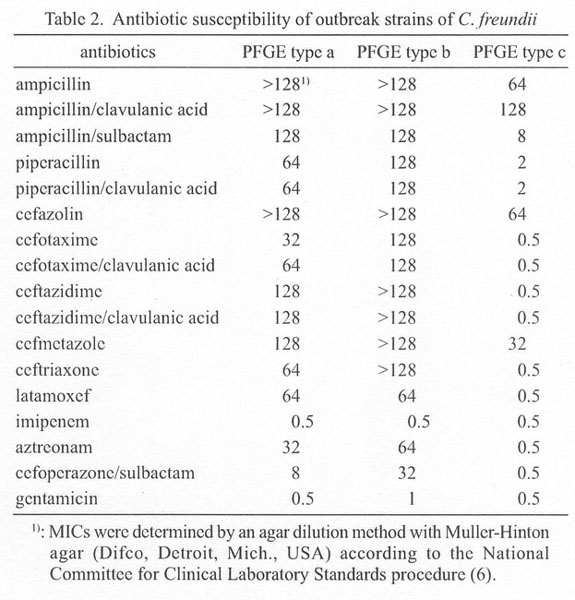
We report here a small outbreak of infection caused by third generation cephem-resistant C. freundii on a surgical ward of a university hospital in 2002. We identified four patients with biliary infection and two carrier patients during July and October. All of the infection cases (patients A, B, E, and F) and one colonization case (patient G) underwent surgical procedures prior to the isolation of resistant C. freundii (Table 1). C. freundii were isolated from bile, wound gauze, ascites, pus, and/or feces of these patients. Epidemiological study using pulsed-field gel electrophoresis (PFGE) revealed that two different PFGE types of strains were involved in the outbreak; PFGE patterns of lanes 1, 2, 3, and 4 were indistinguishable from each other, and the patterns of lanes 5 and 6 were likewise identical (Fig. 1). These types were tentatively designated as a and b, respectively, and strains of both types were found to be highly resistant to third generation cephems including ceftazidime and ceftriaxone, but sensitive to imipenem (Table 2). Type a strain and type b strain showed similar antibiotic susceptibility profiles, suggesting that these strains were evolutionarily related, or that these strains carry similar antibiotic resistant genes on a putative plasmid. The susceptibility profile of type c strain was different from those of type a and b strains.
As previous studies have indicated, third generation cephem-resistance of Gram-negative bacteria are due to the hydrolysis of b-lactams by b-lactamases. These b-lactamases include extended spectrum b-lactamase (ESBL), metallo-b-lactamase, and plasmid-encoded AmpC cephalosporinase (1-3). ESBL confers variable levels of resistance to cefotaxime, ceftazidime, and other broad-spectrum cephalosporins and to monobactams, but has no detectable activity against cephamycins and carbapenems, and is relatively sensitive to sulbactam (1). Plasmid-encoded metallo-b-lactamase hydrolyzes imipenem as well as almost all penicillins and cephems (2). Plasmid-encoded AmpC cephalosporinases of Gram-negative bacteria are uncommon and have broad substrate specificity including cephamycins but not carbapenems, as compared with chromosomally encoded AmpC cephalosporinases (3-5). Types a and b C. freundii strains were resistant to cephamycins and b-lactamase inhibitors, and were sensitive to imipenem. It is therefore likely that these third generation cephem-resistant C. freundii strains carry a plasmid-encoded AmpC cephalosporinase that hydrolyzes new cephalosporins and cephamycins. However, conjugational studies to transfer the resistances of type a and b C. freundii strains to Escherichia coli raised no resistant transconjugants, indicating that the resistance to new third generation cephems is rather chromosomal. Attention to nosocomial spread of Gram-negative bacteria that carry this type of resistance is recommended.
REFERENCES
{kind=link}
{kind=link}
{kind=link}