Jpn. J. Infect. Dis., 57, 86-88, 2004
To see a printable version of the article in the Adobe file format, click this [PDF] link.
Laboratory and Epidemiology Communications
Molecular Epidemiology of Methicillin-Resistant Staphylococcus aureus in a Kumamoto Hospital in 2003
Fumio Kawano*, Hisayoshi Miyazaki, Tatsuya Kawasaki, Tomoko Fujinol, Jun-ichiro Sekiguchil, Katsutoshi Sarutal, Tadatoshi Kuratsujil and Teruo Kirikael
National Hospital Organization, Kumamoto National Hospital, Kumamoto 860-0008 and 1International Medical Center of Japan, Tokyo 162-8655
Communicated by Hiroshi Yoshikura
(Accepted March 25, 2004)
*Corresponding author: Mailing address: Kumamoto National Hospital, Ninomaru 1-5, Kumamoto 860-0008, Japan. Fax: +81-96-325-2519. E-mail: f-kawano@sa2.so-net.ne.jp
Methicillin-resistant Staphylococcus aureus (MRSA) is a prevalent nosocomial pathogen in healthcare facilities. Epidemiological analysis of MRSA isolates assisted by analysis of restriction fragment length polymorphisms of genomic DNA using pulsed-field gel electrophoresis (PFGE) is essential for achieving hospital infection control (1-3).
Sixty-seven MRSA isolates were obtained from 35 inpatients during October 2003 in a hospital with 11 wards and 550 beds in Kumamoto Prefecture. Of these, 34 isolates, each derived from a single patient, were analyzed for chromosomal DNA typing by using the following: a contour-clamped homogeneous electric field system (CHEF MapperTM: Bio-Rad Laboratories, Hercules, Calif., USA), antibiotic resistance (VITEKTM: bioMerieux, Marcy-l'Etoile, France), enterotoxin serotyping (SET-RPLA: Denka Seiken Co., Tokyo), toxic shock syndrome toxin-1 (TSST-1) production (TST-RPLA: Denka Seiken), coagulase serotyping (Denka Seiken).
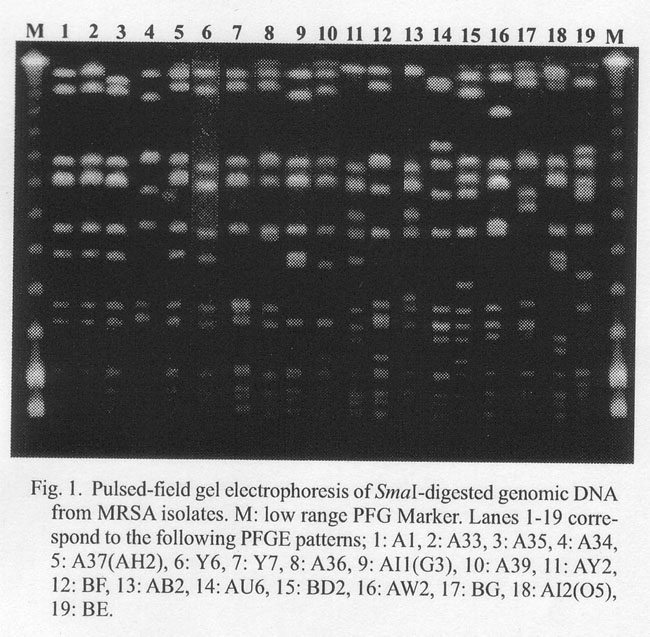
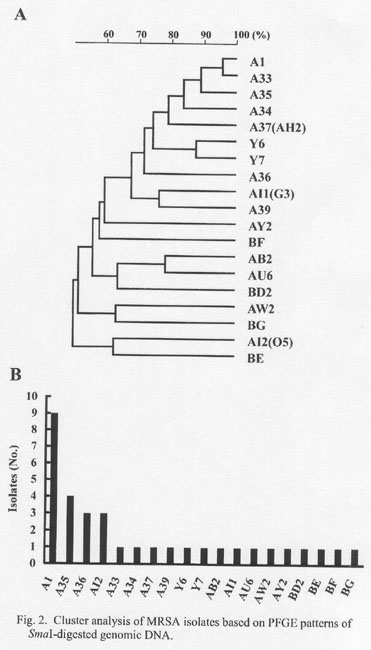
Nineteen different PFGE patterns of SmaI DNA digests were detected (Fig. 1). A band-based cluster analysis (Molecular AnalystTM: Bio-Rad) revealed 10 clusters, A/Y, AI/A, AY, BF, AB/AU, BD, AW, BG, AI, and BE (patterns with more than 70% similarity were considered to form a cluster) (Fig. 2A). The frequency distribution of the PFGE patterns of MRSA is shown in Fig. 2B. The most frequent pattern (A1) represented 26% of the total isolates. Pattern A35 was detected in four isolates, patterns A36 and AI2 in three isolates. The remaining 15 patterns were identified in one isolate each.
MRSA with the pattern A1 was isolated from different wards as follows: one isolate was in the critical care center, two in ward e1, one in ward a1, two in ward a3, and three in ward a6. MRSA isolates with patterns A35, A36, and AI2 were detected in two or more wards. Four MRSAs with the pattern A35 were isolated from ward e2, ward a1, the intensive care unit, and the critical care center; three isolates with the pattern A36 were from ward a6 and the critical care center, and three isolates with the pattern A12 (O5) were from ward a5 and the critical care center (Table 1). These results appear to suggest the multi-focal clonal expansion of MRSA in this hospital.
Sensitivity to antibiotics is shown in Table 2. The MRSA isolates were resistant to 9-12 of 15 drugs tested. All of the isolates were sensitive to arbekacin, vancomycin, and teicoplanin. Nine isolates having the PFGE pattern A1 had antibiotic pattern a or c. No correlation was found between antibiotic resistance and PFGE pattern.
All of the 34 MRSA isolates produced coagulase type II and TSST-1. Thirty-one isolates produced enterotoxin type C, one isolate produced enterotoxin types A and C, and one isolate produced enterotoxin types C and D. Collectively, among 34 MRSA isolates, 31 produced coagulase type II, enterotoxin type C, and TSST-1; i.e., most of the isolates shared common characteristics in terms of these parameters.
PFGE-based MRSA surveillance was conducted in the same hospital in October 2001 (1), October 2002 (2), and in a hospital in Tokyo in October 2003 (3). In these surveillance studies, a total of 56 PFGE patterns were detected (Fig. 3). PFGE patterns A1 and AI2(O5) were detected in Kumamoto in all of these surveillance studies conducted in 2001, 2002, and 2003. PFGE pattern A37(AH2) was detected in Kumamoto in 2002 and 2003. PFGE pattern Y4(A6) was detected in Kumamoto in 2001 and 2002. The other patterns were unique to each year (Fig. 3) (1,2). Pattern A33 was a newly detected pattern in the present study and was nearly identical to pattern A1, except the top band showed slightly slower migration. The present study indicates the co-existence of persistent and rapid turnover of MRSA in the hospital setting. Pattern A1 was detected in a hospital in Kumamoto in 2001, 2002, and 2003, and this pattern was also detected in a hospital in Tokyo (3). Among the patterns identified here, pattern A1 was most frequently detected in both hospitals (Fig. 2B) (3). The present data indicate the clonal expansion of MRSA, not only within hospitals, but also nationwide.
REFERENCES
Go to JJID Homepage Go to JJID 57(2) Contents
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}