Jpn. J. Infect. Dis., 54, 117-118, 2001
To see an article, click this [PDF] link.
Laboratory and Epidemiology Communications
Molecular Epidemiology of Methicillin-Resistant Staphylococcus aureus in a Community Hospital in Hiroshima
Junko Kawasaki, Tomoko Fujino1, Yoshikazu Naiki1, Namiko Mori1, Rie Sasaki, Norikazu Shigeto and Teruo Kirikae1*
National Hataka Hospital, Hataka 2-14-1, Aki, Hiroshima 736-0088
and
1International Medical Center
of Japan, Toyama 1-21-1, Shinjuku-ku, Tokyo 162-8655
Communicated by Hiroshi Yoshikura
(Accepted June 20, 2001)
Methicillin-resistant Staphylococcus aureus (MRSA) is a major nosocomial pathogen in hospitals, including community hospitals with relatively small number of beds (1). Restriction fragment length polymorphism analysis of genomic DNA using pulsed-field gel electrophoresis (PFGE) is a powerful tool for assessment of hospital infection controls (2).
The present study was conducted in a hospital in Hiroshima with two wards and 100 beds. In August 2000, MRSA was isolated from five patients' sputa in ward I and three patients' sputa and one patient's stool specimen in ward II. In December, MRSA was isolated from five patients' sputa and one patient's pus in ward I and two patients' sputa in ward II. At the time, a MRSA survey of the hospital personnel was performed and five carriers were detected, including a doctor and four nurses, among eight doctors and forty-three nurses. The isolates from the patients and the carriers were tested for chromosomal DNA typing by using a contour-clamped homogeneous electric field system (CHEF MapperTM, Bio-Rad Laboratories, Hercules, Calif., USA), enterotoxin serotyping (SET-RPLA, Denka Seiken Co., Tokyo), toxic shock syndrome toxin-1 (TSST-1) production (TST-RPLA, Denka Seiken), and coagulase serotyping (Denka Seiken).
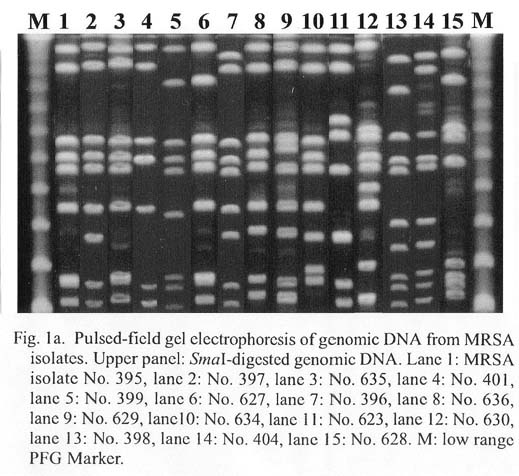
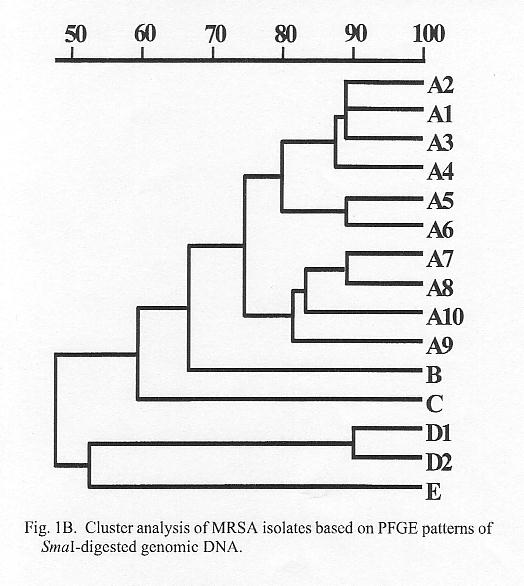
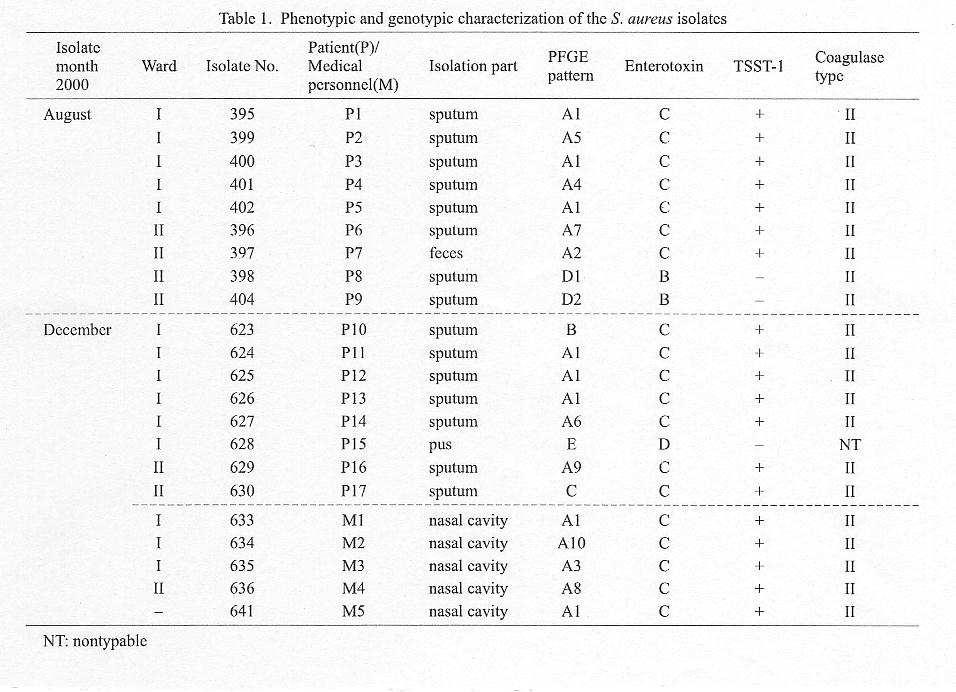
Fifteen different PFGE patterns of SmaI DNA digests were detected (Fig. 1a). Band-based cluster analysis of these patterns (Molecular AnalystTM, Bio-Rad) revealed five clusters A to E (Fig. 1b) (patterns sharing a similarity of 70% or higher were grouped into a cluster). Patterns B and C exhibited more than 60% similarity to patterns A and D. E shared less similarity with the others (Fig. 1b). MRSA isolates with PFGE pattern A (Nos. 395, 396, 397, 399, 400, 401, 402, 624, 625, 626, 627, 629, 633, 634, 635, 636, and 641), and isolates with patterns B (No. 623) and C (No. 630) produced enterotoxin type C, TSST-1, and coagulase type II (Table 1). Isolates with PFGE pattern D (Nos. 398 and 404) produced enterotoxin type B and coagulase type II, but did not produce TSST-1 (Table 1). An isolate with pattern E (No. 628) produced enterotoxin D and nontypable enterotoxin other than types A, B, C, or D (Table 1).
All of the five MRSA isolates from ward I in August were of cluster type A and producers of enterotoxin type C, TSST-1, and coagulase type II. Four of six isolates from the same ward in December were of the same type, and all the clinical personnel (M1-M5) carried MRSA of the same type. MRSA of the same type was isolated in ward II in August (Nos. 396 and 397) and December (No. 629). The above observation appears to suggest that the main MRSA infections during the observation period were initiated by a single MRSA strain which mainly spread in ward I through medical personnel or other vehicles.
REFERENCES
*Corresponding author: Fax: +81-3-3202-7364, E-mail: tkirikae@ri.imcj.go.jp
Go to JJID Homepage Go to JJID 54(3) Contents
{kind=link}
{kind=link}
{kind=link}