Jpn. J. Infect. Dis., 54, 121-122, 2001
To see an article, click this [PDF] link.
Laboratory and Epidemiology Communications
Changing Patterns of Serotypes and Antimicrobial Susceptibilities of Shigella Species Isolated from Children in Calcutta, India
Swapan Kumar Niyogi*, Utpala Mitra and Phalguni Dutta
Division of Microbiology and Clinical Medicine, National Institute of Cholera & Enteric Diseases, P33 CIT Road Schm XM, P O Beliaghata, Calcutta 700 010, India
Communicated by Haruo Watanabe
(Accepted July 17, 2001)
Shigellosis occurs both in epidemic and endemic forms in children and remains a major public health problem in developing countries. Over the past decades, Shigella spp. have become progressively resistant to most of the widely used and inexpensive antimicrobials (1). Moreover, changes in the incidence of Shigella subgroups from time to time makes it difficult to formulate a drug of choice for shigellosis (2). The present study reports the distribution of Shigella subgroups and the antimicrobial susceptibility pattern of Shigella spp. isolated from children in Calcutta, India.
From January 1998 to December 2000, a total of 675 stool samples were collected from children suffering from acute diarrhea attending the Diarrhoea Treatment Unit at Dr. B.C. Roy Memorial Hospital for Children, Calcutta, and were cultured for Shigella spp. All isolates were confirmed serologically by slide agglutination using commercially available specific antisera (Denka Seiken, Tokyo). Antimicrobial susceptibility tests were performed using an agar diffusion technique method following National Committee for Clinical Laboratory Standards guidelines (3).
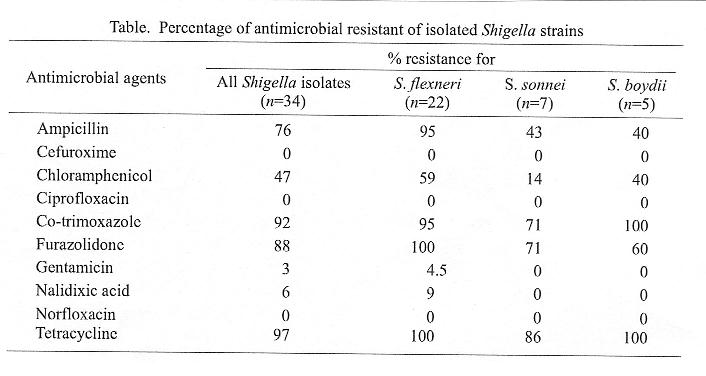
The thirty-four strains of Shigella spp. that were isolated were distributed as follows: 22 (65%) were S. flexneri, 7 (2.0%) were S. sonnei and 5 (15%) were S. boydii. No S. dysenteriae strains were isolated. The antimicrobial susceptibility pattern of Shigella strains is shown in Table.
Temporal and spatial variations in the isolation of Shigella spp. have been reported in various parts of India from time to time. Before 1984, S. flexneri was the predominant species isolated sporadically from 3% of diarrhea cases in Calcutta (4). S. dysenteriae type 1, the most virulent and epidemic potential serotype, was not isolated in that period. In 1984, an epidemic of shigellosis caused primarily by S. dysenteriae type 1 broke out in the eastern parts of India affecting thousands of people and caused many deaths in and around Calcutta (5). During the epidemic of bacillary dysentery (1984), isolation of Shigella spp. as well as S. dysenteriae type 1 was high. Decreased isolation of S. dysenteriae type 1 and increased isolation of S. flexneri was observed during post-endemic years (6). However, during 1990-1992 S. dysenteriae type 1 was isolated more from Calcutta (7). During the period 1995-1996 in a study conducted among children, S. flexneri was isolated as predominant serotype (51%) followed by S. boydii (21%), S. sonnei (17%), and S. dysenteriae type 1 (10%), respectively (8). During the 1984 epidemic highly encouraging results through the use of nalidixic acid in the treatment of multi-resistant S. dysenteriae type 1 infection was reported from Calcutta (9). However, within s short period the widespread use of the drug resulted in the emergence of a nalidixic acid-resistant S. dysenteriae type 1 strain in several parts of the world including India (10), negating the efficacy of the drug. A study conducted in our institute during 1990-1992 demonstrated a significantly low resistance to nalidixic acid and furazolidone (7). During 1995-1996, however, increased resistance to nalidixic acid and furazolidone was observed (8). In the present study, a significantly low resistance to nalidixic acid was observed. The development of resistance to furazolidone steadily increased over the past few years (8) and we also observed a markedly high resistance to furazolidone.
The shift in the prevalence of serogroups and the changing pattern in antimicrobial susceptibilities among Shigella isolates poses a major difficulty in the determination of an appropriate drug for the treatment of shigellosis. Continuous monitoring of antimicrobial susceptibilities of Shigella spp. through a surveillance system is thus essential for effective therapy and control measures against shigellosis.
Authors thank Mr. S. K. Das for typing the manuscript.
REFERENCES
*Corresponding author: Tel: +91-33-350-0448, Fax: +91-33-350-5066, E-mail: niced@cal2.vsnl.net.in
Go to JJID Homepage Go to JJID 54(3) Contents
{kind=link}