Jpn. J. Infect. Dis., 54, 125-126, 2001
To see an article, click this [PDF] link.
Laboratory and Epidemiology Communications
Seroprevalence of Human Herpesvirus 8 in Okinawa, Japan
Masao Satoh*, Hiromu Toma1, Yoshiya Sato1, Chotaku Futenma2, Susumu Kiyuna3, Yoshiyuki Shiroma3, Akatsuki Kokaze4, Shinsaku Sakurada5, Tetsutaro Sata6 and Harutaka Katano6
Department of Medical Zoology, Saitama Medical School, Morohongo, Moroyama, Iruma-gun, Saitama 350-0495, 1Department of Parasitology, School of Medicine, University of the Ryukyu, Uehara 207, Nishihara, Okinawa 903-0125, 2Minamidaito Clinic, Zaisho 183-1, Minamidaito, Shimajiri-gun, Okinawa 901-3805, 3Izumizaki Hospital, Izumizaki 1-11-2, Naha, Okinawa 900-0021, 4Department of Public Health, Kyorin University School of Medicine, Shinkawa 6-20-2, Mitaka-shi, Tokyo 181-8611, 5Bureau of International Cooperation, International Medical Center of Japan, Toyama 1-21-1, Shinjuku-ku, Tokyo 162-8655 and 6Department of Pathology, National Institute of Infectious Diseases, Toyama 1-23-1, Shinjuku-ku, Tokyo 162-8640
Communicated by Tetsutaro Sata
(Accepted July 27, 2001)
The human herpesvirus 8 ([HHV-8], Kaposi's sarcoma [KS]-associated herpesvirus, [KSHV]) DNA sequence has been demonstrated in all forms of KS, which is the most common malignant tumor among patients with acquired immunodeficiency syndrome (AIDS) (1,2). It was also shown that the virus encoded several genes homologous to cell cycle-associated genes and cytokines, suggesting that HHV-8 infection is necessary for the development of KS (3). The geographic distribution of KS in the world is restricted to certain regions (4,5), and this geographic clustering could result from as-yet-undefined genetic or environmental factors. Although patients with KS are rare in Japan (6), some cases of KS have been observed in Okinawa, which is located in the southern islands of Japan (7,8). Since Okinawa is an endemic area of human T-cell leukemia virus type I (HTLV-1), some KS cases in Okinawa have been associated with adult T cell leukemia/lymphoma or AIDS. However, cases of the classic type KS have been also reported from this area (7); therefore, Okinawa is suspected to be one of the endemic areas of KS. The seropositivity rate of anti-HHV-8 antibodies in the general Japanese population has been reported at 1.4% (9); however, the seroprevalence in Okinawa has not yet been studied. In this study, to clarify the factors involved in the development of KS in Okinawa, the seropositivity rate of anti-HHV-8 antibodies was examined compared to the general Japanese population.
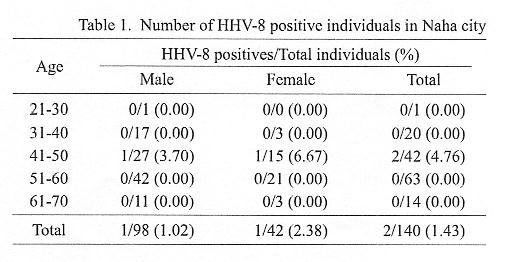
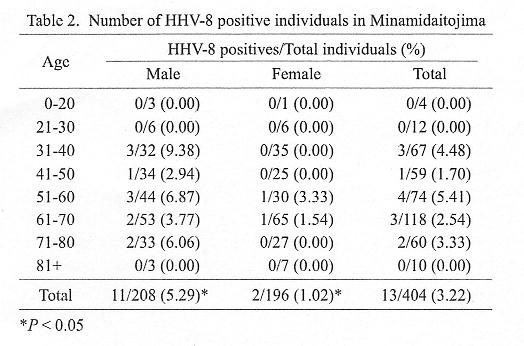
To study the distribution of HHV-8 carriers in Okinawa, we examined the positivity rate of anti-HHV-8 antibody in the serum. Sera were collected from a total of 140 individuals (98 males and 42 females) during health examinations in Naha city, which is the central city of the main island of Okinawa, and a total of 404 individuals (208 males and 196 females) in Minamidaitojima, a smaller island which is about 300 km distant from Naha city. The ages (mean Å} SD) were 49.8 Å} 9.01 (male) and 51.2 Å} 6.68 (female) in Naha city, and 55.6 Å} 14.9 (male) and 56.8 Å} 15.5 (female) in Minamidaitojima. Informed consent was obtained from all individuals. All sera were stored at -20Åé and heat inactivated at 56Åéfor 30 min before use. The presence of anti-HHV-8 antibodies was determined by a mixed-antigen enzyme-linked immunosorbent assay (using K8.1, ORF59, ORF65 and ORF73 proteins as mixed antigens) and indirect immunofluorescence assay using acetone-fixed TY-1 cells (HHV-8-positive primary effusion lymphoma cell line) (9,10). Fisher's exact probability test was used to analyze the significance of differences.
Only two positives were found in 140 individuals (1.43%) in Naha city (Table 1). This positivity rate was almost the same as that reported in the general Japanese population (9). On the other hand, 13 positives were found in 404 individuals (3.22%) in Minamidaitojima (Table 2). This seropositivity rate was found to be slightly higher than that of the general Japanese population. This was due to an increased seropositivity rate of males. Seropositivity of males in Minamidaitojima showed two peaks, one in the older groups (over 50 years old), and the other in 30 to 40 years old. There were only 2 female seropositive individuals in the elders. The reason why the positive rate of HHV-8 in Minamidaitojima, especially in younger males, was higher than that in Naha city and the general Japanese population is not clear. Because Minamidaitojima is a small island and far away from the main island of Okinawa, the population on this island is relatively isolated. Angeloni et al. (11) reported the familial transmission of HHV-8. The two peaks of positive groups in males might support this possibility. However, because the age distribution in Minamidaitojima was older than that of the general Japanese population (9), the differences in seropositivity rates could not be conclusively explained.
In conclusion, non-significant differences in the seropositivity rates of anti-HHV-8 antibodies were observed between the Okinawa population and the general Japanese population in this study. Events in addition to HHV-8 infection, such as environmental factors, may be needed for the development of KS in Okinawa.
REFERENCES
Go to JJID Homepage Go to JJID 54(3) Contents
{kind=link}
{kind=link}