Jpn. J. Infect. Dis., 54, 128-129, 2001
To see an article, click this [PDF] link.
Laboratory and Epidemiology Communications
Prevalence of Adenovirus Types 3 and 7 Antibodies
in Singapore
Osamu Nishio*, Kiyohiko Matsui, Kee-tai Goh1,
Yasuko Matsunaga2 and Sakae Inouye2,3
Department of Microbiology, National Institute of Public Health, Shirokanedai 4-6-1, Minato-ku, Tokyo 108-8638, 1Quarantine & Epidemiology Department, Ministry of the Environment, Singapore, 2Infectious Disease Surveillance Center, National Institute of Infectious Diseases, Tokyo and 3Otsuma Women's University, Tokyo
Communicated by Sakae Inouye
(Accepted August 2, 2001)
Adenovirus types 3 and 7 (Ad3 and Ad7), which belong to subgenus B of human adenovirus, cause both acute keratoconjunctivitis and respiratory-tract infections. Particularly, Ad7 is known to elicit lethal pneumonia in children with a basal ailment in the heart or lung (1). In Japan, Ad7 began to be isolated in 1995 (2,3) and it raised a great concern among pediatricians because the number of Ad7 isolation reports increased during 1996-1998 accompanying serious cases (4); however, the isolation decreased in 1999 and 2000 (4).
To investigate the epidemiology of Ad3 and Ad7 infections in Japan, we previously conducted a retrospective serosurvey (5) using sera stored in Serum Bank, National Institute of Infectious Diseases, and found that the Ad7 antibody-prevalence rates were less than 10% among <15-year-olds in the sera collected in 1974-1975 but they were low among <40-year-olds in the sera collected in 1993-1994, indicating that the people up to the age of 40 had not experienced Ad7 infection in 1993-1994. In contrast, we found that the Ad3 seroprevalence curves are quite similar between the 1970s and the 1990s: the prevalence curves rise up from the youngest age. Thus we postulated that Ad7 had not prevailed in Japan since the late 1950s or early 1960s while Ad3 had been present all the time (5).
In the present study, we conducted a serosurvey using sera collected in Singapore in 1992 and compared the results with those of Japan. We used sera collected from 545 persons at the age of 1 to 69 years living in Singapore. Neutralizing antibodies to Ad3 and Ad7 were assayed with use of the HEp-2 cells, as previously described (5). Antibody titers of 1:4 or over were regarded as antibody positive.
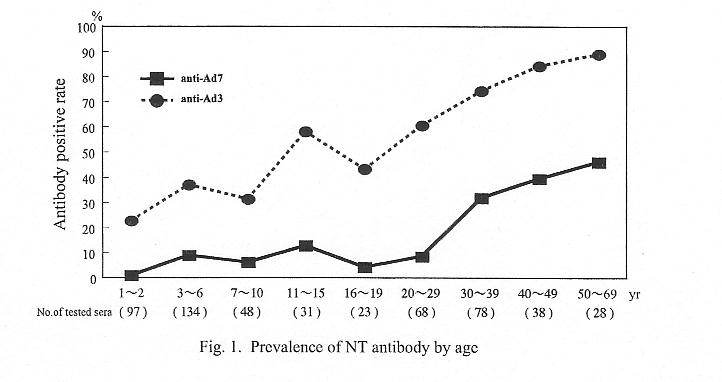
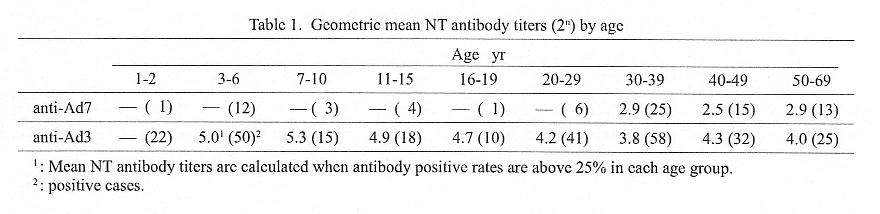
Figure 1 shows the age-specific seroprevalence curves of Ad3 and Ad7. Anti-Ad7 prevalence rates were low among <30-year-olds, whereas anti-Ad3 prevalence increased from the youngest age. Table 1 shows geometric mean antibody titers among antibody positives in different age groups. Ad3 antibody titers in young age groups were higher than those in older age groups; Ad7 antibody titers among üå30-year-olds were low (22.5 to 22.9). These results were found to be similar to the antibody prevalence patterns and mean antibody titers of the sera collected in 1982-1983 in Japan (5).
The above seroepidemiologic data suggest that the Ad7 infection had not been endemic for a few decades in Singapore before the time of the serum collection (1992), although Ad7 was sporadically isolated in the 1980s (6). Recently from 1994, however, at Singapore General Hospital, some numbers of Ad7 have been isolated (7). Once Ad7 is introduced into Singapore, it may spread among non-immune young people. A close watch is needed in order to prevent Ad7 nosocomial infections in pediatric wards.
REFERENCES
*Corresponding author: E-mail: nishio@iph.go.jp
Go to JJID Homepage Go to JJID 54(3) Contents
{kind=link}
{kind=link}