Jpn. J. Infect. Dis., 54, 151-152, 2001
To see an article, click this [PDF] link.
Laboratory and Epidemiology Communications
Pulmonary Mycobacterium avium Infection in an Immunocompetent Young Adult Related to Use of Home Bath with a Circulating Water System
Aya Watando, Emiko Toyota*, Namiko Mori, Aki Kaneko, Tadatoshi Kuratsuji, Teruo Kirikae and Koichiro Kudo
International Medical Center of Japan, Toyama 1-21-1, Shinjuku-ku, Tokyo 162-8655
Communicated by Hiroshi Yoshikura
(Accepted August 13, 2001)
Unsuitable management of bath water occasionally causes waterborne infectious diseases, such as legionellosis and infections due to non-tuberculosis mycobacteria. (The draft guideline is available with the full text of this article at http://www.cdc.gov/ncidod/hip/enviro/env_guide_draft.pdf )(1).
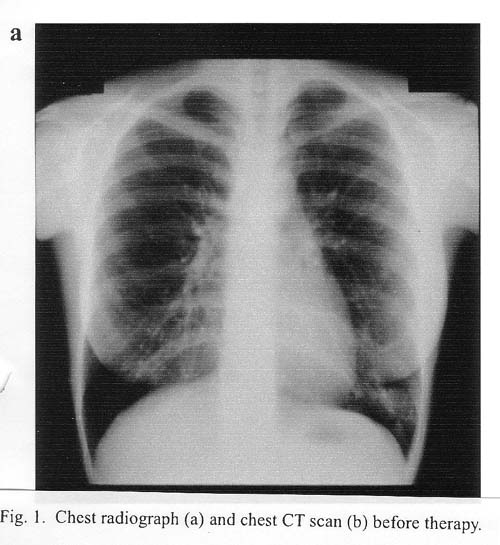
A 21-year-old female student (patient A) was referred to the corresponding author in May 2000, with a routine chest radiograph revealing left lobe shadowing, and with mild fever and a productive cough that had continued since March. She was a nonsmoker. She had a history of Mycoplasma pneumoniae infection at 12 years of age. At hospitalization, a tuberculin skin test was negative (0 x 0 induration with 9 x 8 mm of redness), and a test for HIV antibody was also negative. The lungs were clear with no crackles or wheezes. Routine laboratory tests disclosed no abnormalities.
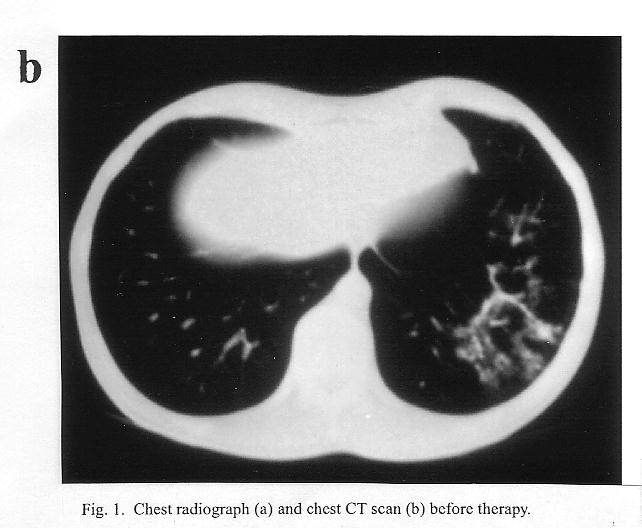
A chest radiograph revealed left lower lobe consolidation (Fig. 1a). A CT scan revealed an infiltration with thickened wall of left B9 (Fig. 1b). Her sputum smear was acid-fast bacilli (AFB) negative. However, by diagnostic tests based on polymerase chain reaction (PCR) (COBAS AMPLICORTM MTB, M. avium and M. intracellulare tests: Roche Diagnostics, Branchburg, N.J., USA), the sputum was positive for M. avium. It was, however, negative for M. tuberculosis and M. intracellulare. The bronchial aspirates were AFB and M. avium complex (MAC) culture positive. Four drug chemotherapy consisting of clarithromycin, rifampin, streptomycin, and ethambutol was started immediately. The MAC isolate was resistant to rifampin (MIC: >50 mg/ml), streptomycin (MIC: >20 mg/ml), and ethambutol (MIC: >5 mg/ml), but relatively sensitive to clarithromycin (MIC: 4 mg/ml). After 3 months of treatment, she became asymptomatic, and her chest radiograph and CT scan improved.
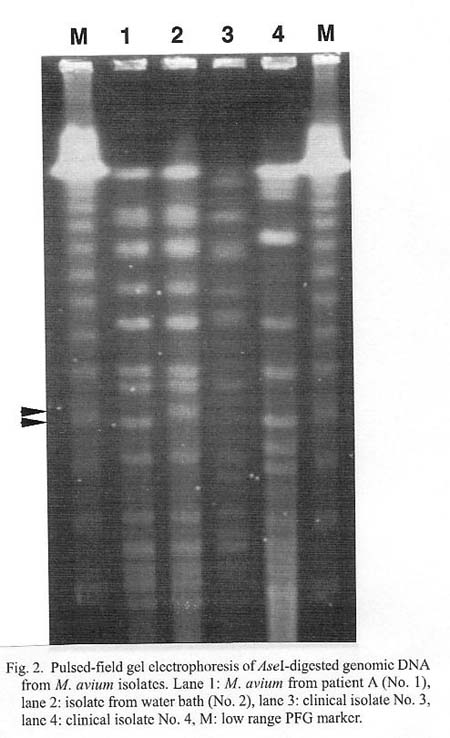
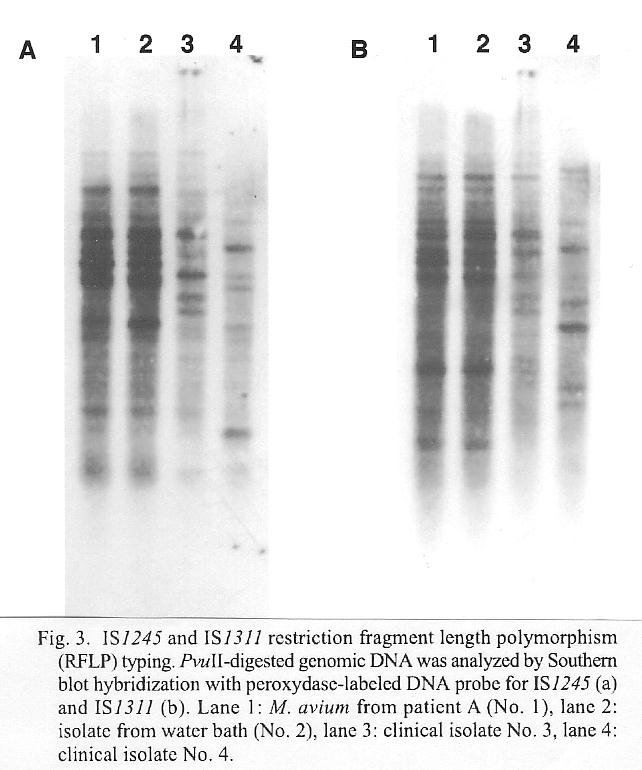
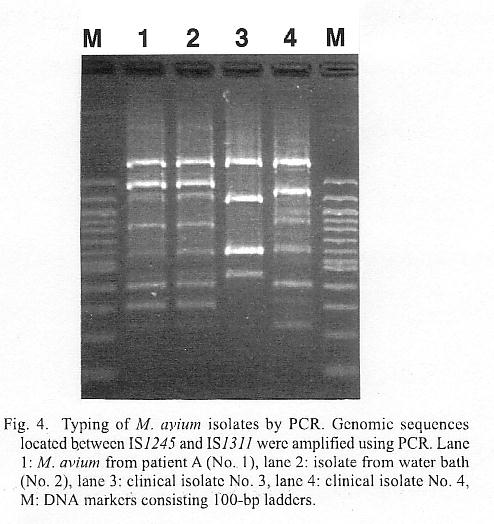
The patient and her family used a bath with a circulating and filtering water system in their home. The bath water was found MAC culture positive. PCR-based diagnosis revealed that the MACs both from the bath water and the patient were M. avium. To determine whether these isolates were derived from a clone, chromosomal DNA's derived from these two isolates and two more M. avium clinical isolates not associated with the present case were analyzed by pulsed-field gel electrophoresis (PFGE) (CHEF MapperTM: Bio-Rad Laboratories, Hercules, Calif., USA) of AseI digests (Fig. 2), IS1245 restriction fragment length polymorphism (RFLP) typing (2) (Fig. 3a), IS1311 RFLP typing (3) (Fig. 3b), and typing based on length polymorphism of ribosomal DNA spacer regions between repetitive IS1245 and IS1311 (LPRS) (4) (Fig. 4).
The PFGE pattern of the lung specimen from patient A (No. 1) and that of the bath water-derived specimen (No. 2) were identical except for one band differenence in size (indicated by an arrow in Fig. 2). Meanwhile, other two clinical isolates (Nos. 3 and 4) were entirely different from isolates Nos. 1 and 2 in PEGE pattern. The patterns obtained by IS1245 RFLP, IS1311 RFLP and LPRS were identical for the patient A's isolate and the bath water-derived isolate (Figs. 3 and 4). Isolates Nos. 3 and 4 showed entirely different patterns from isolate Nos. 1 and 2 in all the assays (Figs. 3 and 4). The data indicated that the M. avium isolate from patient A and that from bath water were of the same clone. Probably, patient A acquired the M. avium infection from the bath water. It remains unknown why only patient A, but not other family members, contracted the disease.
REFERENCES
*Corresponding author: Fax: +81-3-3202-7364, E-mail: etoyota@imcj.hosp.go.jp
Go to JJID Homepage Go to JJID 54(4) Contents
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}