Jpn. J. Infect. Dis., 54, 157-159, 2001
To see an article, click this [PDF] link.
Laboratory and Epidemiology Communications
An Outbreak of Methicillin-Resistant Staphylococcus aureus (MRSA) in a Tuberculosis Ward
Namiko Mori, Hiroshi Kawata, Toshio Hama, Tomoko Fujino, Hisashi Kawahata, Akihiko Kawana, Tamiko Suzuki, Fumiko Yamanishi, Tadatoshi Kuratsuji, Koichiro Kudo, Oichirou Kobori, Yoshio Yazaki and Teruo Kirikae*
International Medical Center of Japan, Toyama 1-21-1, Shinjuku-ku, Tokyo 162-8655
Communicated by Hiroshi Yoshikura
(Accepted September 12, 2001)
Methicillin-resistant Staphylococcus aureus (MRSA) is one of the most important nosocomial pathogens, which are spread primarily by direct or indirect person-to-person contact (1). Genome typing using pulsed-field gel electrophoresis (PFGE) is a powerful tool for investigating the source, transmission, and spread of MRSA.
In June 2001, an MRSA outbreak occurred in one of two tuberculosis wards of a 925-bed hospital. The tuberculosis ward has 42 beds and 32 medical staff members, including doctors, nurses and assistant nurses, routinely working in the ward. Two patients (P1 and P3) developed severe sepsis. MRSA was isolated from the patients' blood and sputum, respectively. Sputum or nasal swabs from other 32 patients and nasal swabs from 32 medical staff members were examined for MRSA isolation. MRSA was isolated from 12 patients and a doctor. A total of 15 isolates were obtained and coded as isolates TBW0701.
The isolates TBW0701 were tested for chromosomal DNA typing by using a contour-clamped homogeneous electric field system (CHEF MapperTM: Bio-Rad Laboratories, Hercules, Calif., USA), antibiotic susceptibility (WalkAwayTM: Dade Behring, Deerfield, Ill., USA), enterotoxin serotyping (SET-RPLA: Denka Seiken Co., Tokyo), toxic shock syndrome toxin-1 (TSST-1) production (TST-RPLA: Denka Seiken), and coagulase serotyping (Denka Seiken).
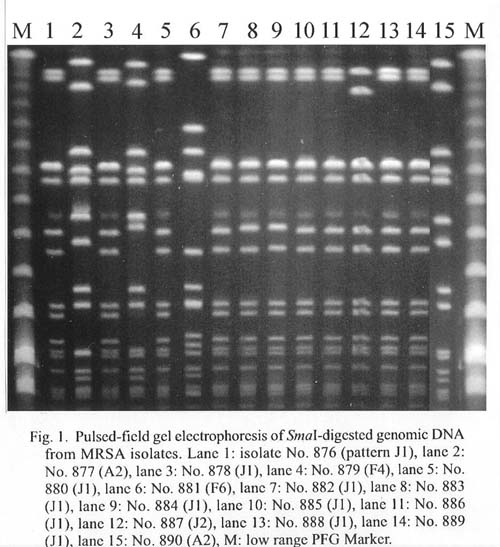
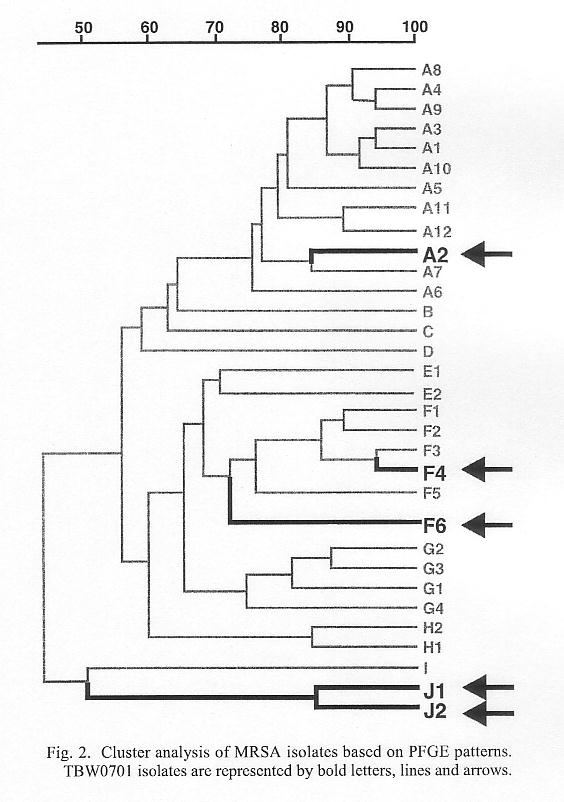
PFGE patterns of SmaI DNA digests of the 15 isolates TBW0701 are shown in Fig. 1. Figure 2 shows cluster band-based analysis of PFGE patterns (Molecular AnalystTM: Bio-Rad) of TBW0701 together with all the MRSA isolates obtained from the same hospital in December 2000 (isolates HOSP1200). Ten clusters, from pattern A to J, are observed if patterns with more than a 70% similarity are postulated to form a cluster (Fig. 2). Isolates HOSP1200 consisted of nine clusters, patterns A to I. Isolates TBW0701 consisted of three clusters, A (A2), F (F4 and F6), and J (J1 and J2). The J cluster was a newcomer which was not found in December 2000.
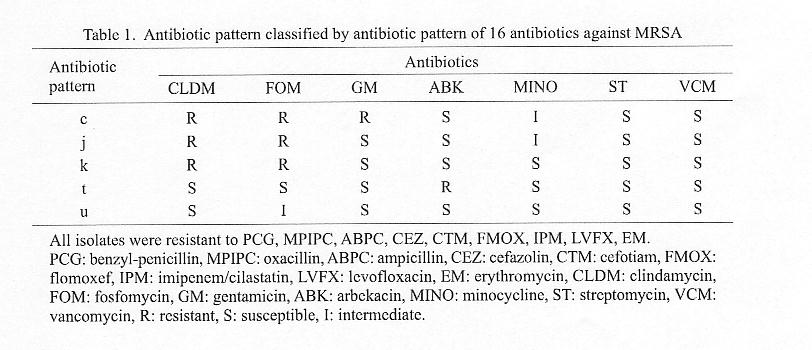
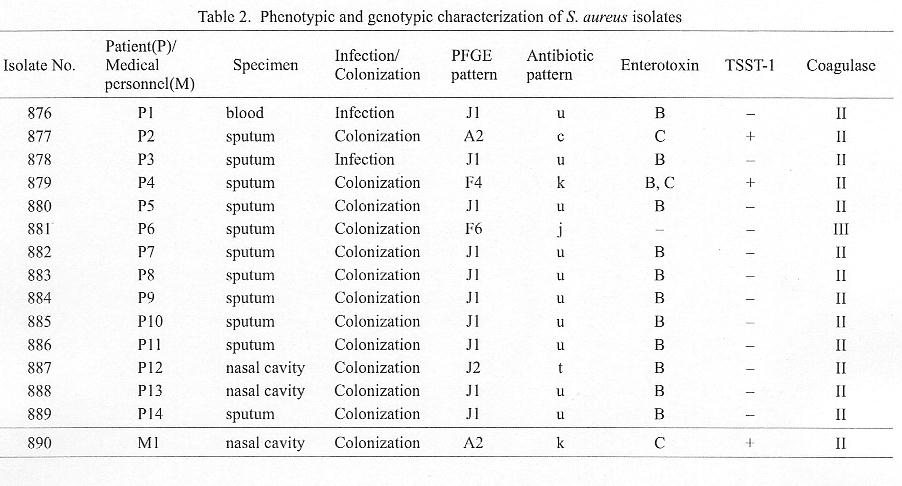
Five different antibiotic sensitivity patterns, c, j, k, t, and u, were seen among isolates TBW0701 (Tables 1 and 2). Among them, eleven strains produced enterotoxin type B, two strains (Nos. 877 and 890) of enterotoxin type C, and one strain (No. 879) of enterotoxin types B and C (Table 2). Isolate No. 881 did not produce any type of enterotoxin. Three strains (Nos. 877, 879, and 890) produced TSST-1. All isolates except No. 881, which produced coagulase type III, produced type II coagulase (Table 2).
It was remarkable that ten TBW0701 isolates (Nos. 876, 878, 880, 882-886, 888, and 889) had the same character (Table 2). They all produced enterotoxin type B, produced coagulase type II, did not produce TSST-1, and had the same PFGE patterns of SmaI DNA digests and the same spectrum of antibiotic susceptibility. They were unique relative to the previous isolates in the following aspects: the isolates had a new PFGE pattern J1 (Table 2 and Fig. 2), produced enterotoxin type B (98% of all hospital isolates produced enterotoxins other than type B) (1), and were TSST-1 negative (96% of hospital isolates were TSST-1 positive) (1). These results indicate that clonal expansion of a new-type MRSA occurred in the tuberculosis ward.
In general, the main mode of transmission of MRSA is via hands, which may become contaminated by contact with colonized or infected persons, or environmental surfaces contaminated with MRSA (2). Most patients in the tuberculosis wards have a higher level of daily activity as compared to other patients, and, as a consequence, share more direct or indirect contact with each other than do patients in other acute health care facilities. However, environmental surfaces in the wards, such as cards, shogi- and go-pieces, a dumbbell, an instrument of foot excise (aotake), a remote TV controller, a catalog for shopping, a tap, a washing machine, a receiver of a public telephone, refrigerator grip, a stethoscope, a keyboard of a personal computer, and a clinical chart, were negative for MRSA culture.
REFERENCES
*Corresponding author: Fax: +81-3-3202-7364, E-mail: tkirikae@ri.imcj.go.jp
Go to JJID Homepage Go to JJID 54(4) Contents
{kind=link}
{kind=link}
{kind=link}
{kind=link}