Jpn. J. Infect. Dis., 54, 159-161, 2001
To see an article, click this [PDF] link.
Laboratory and Epidemiology Communications
Epidemiological Analysis of Nosocomial Outbreaks of Methicillin-Resistant Staphylococcus aureus in a Surgery Ward
Namiko Mori, Tomoko Fujino, Toshitaka Kashima, Jyoji Tomioka, Akihiko Kawana, Hisashi Kawahata, Yoshie Takahashi, Fumiko Yamanishi, Sosuke Kimura, Tadatoshi Kuratsuji, Koichiro Kudo, Oichirou Kobori, Yoshio Yazaki and Teruo Kirikae*
International Medical Center of Japan, Toyama 1-21-1, Shinjuku-ku, Tokyo 162-8655
Communicated by Hiroshi Yoshikura
(Accepted September 17, 2001)
Nosocomial infection, especially postoperative infection caused by methicillin-resistant Staphylococcus aureus (MRSA), is a serious problem in surgical wards (1). Genome typing using pulsed-field gel electrophoresis (PFGE) is a powerful tool for investigating the source, transmission, and spread of MRSA.
In July 2001, an MRSA outbreak occurred in a 42-bed surgical ward of a hospital with 925 beds. Two patients (P2 and P6) developed sepsis, one (P5) had surgical site infection. MRSA was isolated from the patients' blood and the surgical sites. MRSA was also isolated from the sputum of three other patients (P1, P3, and P4) who did not manifest any clinical symptoms due to infections. A total of six isolates were obtained and coded as 2001 outbreak isolates. In the same ward, two MRSA outbreaks had occurred in November to December 1999 (2), and in June to August 2000 (3). Eight different PFGE patterns (MRSA.IMCJ.A3, A5, A6, A7, A10, A11, A12, and B) were found in the former case (2) and five patterns (MRSA.IMCJ.A1, A2, A4, A8, and A9) in the latter case (3).
Chromosomal DNA typing was performed using a contour-clamped homogeneous electric field system (CHEF MapperTM: Bio-Rad Laboratories, Hercules, Calif., USA). The isolates were also tested for antibiotic resistance (WalkAwayTM: Dade Behring, Deerfield, Ill., USA), enterotoxin serotyping (SET-RPLA: Denka Seiken Co., Tokyo), toxic shock syndrome toxin-1 (TSST-1) production (TST-RPLA: Denka Seiken), and coagulase serotyping (Denka Seiken).
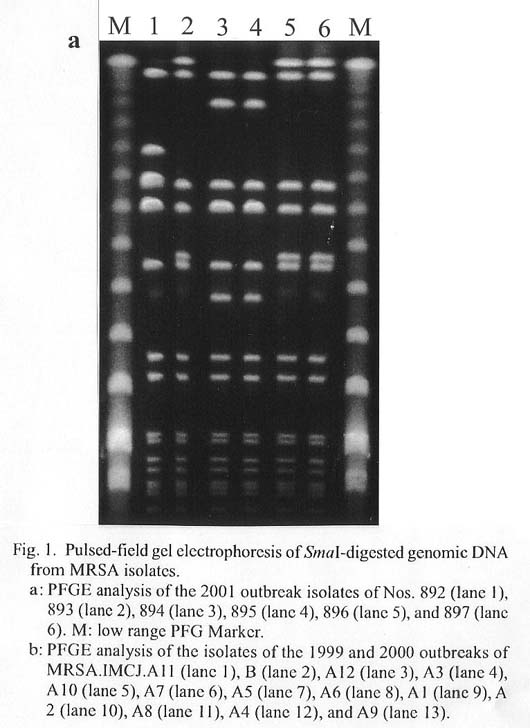
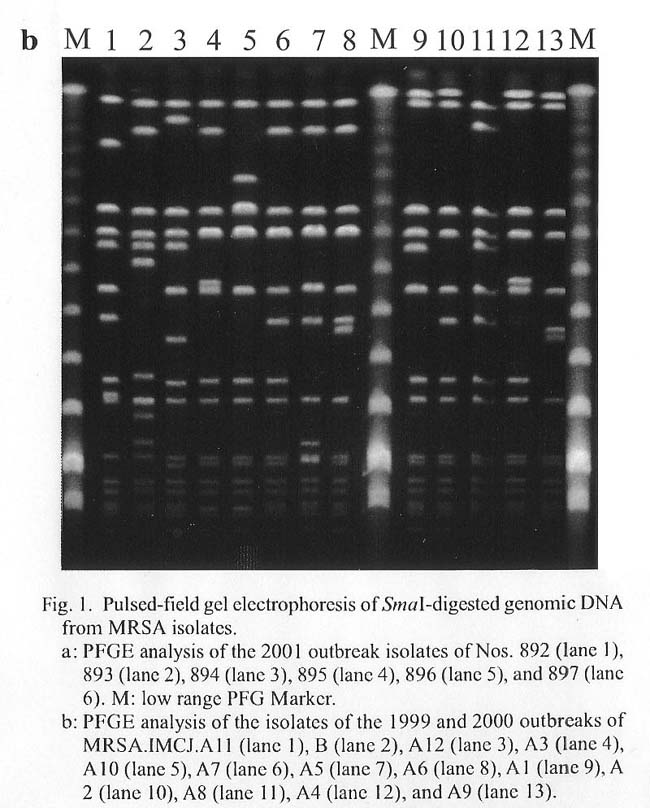
PFGE patterns of SmaI DNA digests of six isolates from the 2001 outbreak and 13 isolates from the 1999 and 2000 outbreaks are shown in Figs. 1a and b. Among the 2001 outbreak isolates, three isolates, Nos. 893, 896, and 897 (lanes 2, 5, and 6 in Fig. 1a), shared the same PFGE pattern. Two isolates, Nos. 894 and 895 (lanes 3 and 4), shared the same pattern but the pattern was different from that of the above three. Isolates of No. 892 had a pattern different from any of the others (Fig. 1a). Three MRSA clones appeared to have participated in the 2001 outbreak.
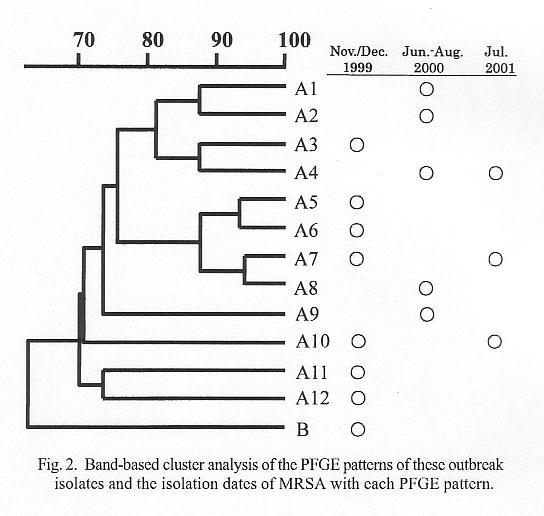
Nos. 893, 896, and 897 had PFGE patterns identical with that of 2000 outbreak isolate A4 (lane 12 in Fig. 1b), Nos. 894 and 895 patterns identical with the 1999 outbreak isolate A7 (lane 6 in Fig. 1b), and No. 892 a pattern identical with the 1999 outbreak isolate A10 (lane 5 in Fig. 1b). The isolation dates of MRSA with each PFGE pattern are shown in Fig. 2. PFGE patterns in the 2001 outbreak are already found in the 1999 and 2000 outbreaks. Band-based cluster analysis of PFGE (Molecular AnalystTM: Bio-Rad) indicated a more than 70% similarity among the isolates in 1999 - 2001 except for pattern B (Fig. 2). This may indicate that MRSA of the same origin persisted in the ward, experiencing small mutations.
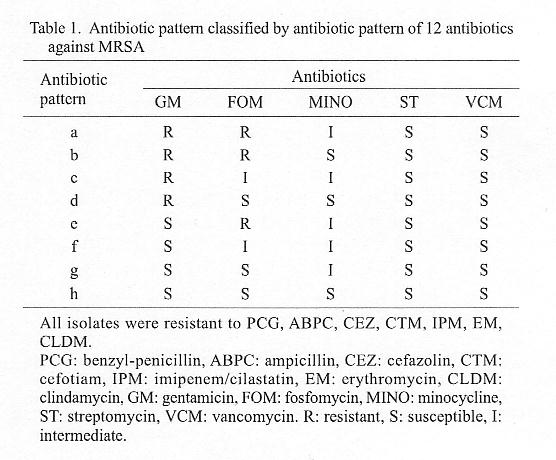
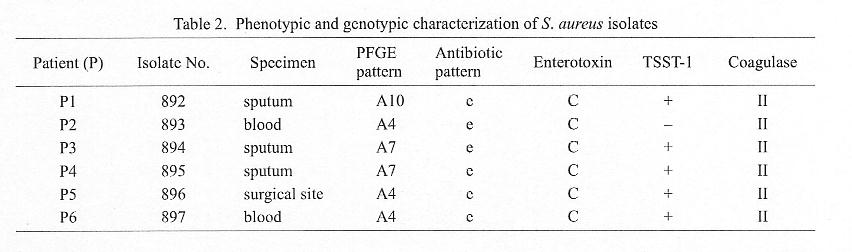
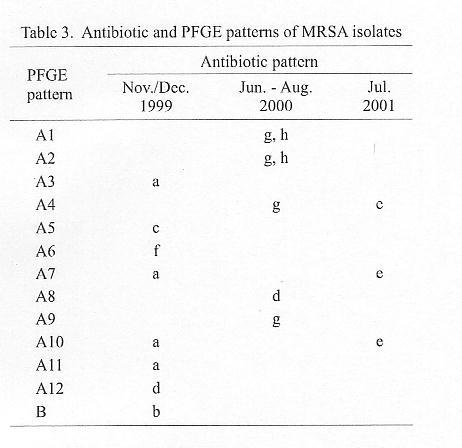
Sensitivity to antibiotics is shown in Tables 1, 2, and 3. All the 2001 outbreak isolates had the same pattern (pattern e, Table 2). The pattern was different from those of the same PFGE pattern isolated at different dates (A4, A7, or A10) (Table 3). This may indicate that antibiotic sensitivity marker is unsuitable for assessing the phylogeny of MRSA. All the 2001 outbreak isolates except No. 893 produced enterotoxin type C, TSST-1 and type II coagulase (Table 2). No. 893 produced enterotoxin type C and type II coagulase, but not TSST-1 (Table 2).
Patients P2, P5, and P6 infected with MRSA with the same PFGE pattern were in different rooms but were treated by a team of doctors. This may indicate the spread of MRSA by medical staff members.
REFERENCES
*Corresponding author: Fax: +81-3-3202-7364, E-mail: tkirikae@ri.imcj.go.jp
Go to JJID Homepage Go to JJID 54(4) Contents
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}