Jpn. J. Infect. Dis., 54, 193-195, 2001
To see an article, click this [PDF] link.
Laboratory and Epidemiology Communications
Isolation of Opportunistic Pathogens in Dental Plaque, Saliva and Tonsil Samples from Elderly
Mohammad Abdus Salam, Hidenobu Senpuku*, Yoshiaki Nomura, Khairul Matin, Hideo Miyazaki1 and Nobuhiro Hanada
Department of Oral Science, National Institute of Infectious Diseases, Toyama 1-23-1, Shinjukuku-ku, Tokyo 162-8640 and 1Division of Preventive Dentistry, Department of Oral Health Science, Graduate School of Medical and Dental Science, Niigata University, Gakkocho-dori 2-5274, Niigata 951-8514
Communicated by Nobuhiro Hanada
(Accepted November 16, 2001)
The oral cavity is a potential reservoir of pathogenic microorganisms (1-3). In the elderly, oral hygiene is poor (4) and dental biofilm containing opportunistic pathogens forms on tooth surfaces (4-6). Oral pathogens are risk factors for bacterial pneumonia as they may be aspirated into the respiratory tract (6,7). Pathogenic bacteria in the biofilm in the dental plaque might also be released to colonize new surfaces, e.g., the tonsils, pharynx, and respiratory tract. To test these possibilities, we studied the isolation frequencies of opportunistic bacteria on tooth and tonsil surfaces, and in saliva in the elderly.
One hundred twenty-five elderly people (mean age: 73.0 Å} 0.3 years old, 66 males and 59 females) from Niigata City in Japan participated in this study, which was conducted in July, 2000. None of the subjects was hospitalized or institutionalized, and all came to the examination center either by themselves or accompanied by their family. They were in good general health and did not require special assistance for their daily activities. Informed consent was obtained from each subject prior to the study. Ethical clearance for the study's methods used was obtained from the Ethics Committee of the Faculty of Dentistry, Niigata University.
Supragingival plaque was collected from the upper right second premolar and first molar teeth by swabbing back and forth with a cotton swab (SEEDSWAB No. 1: Eiken Chemical Co., Ltd. [Eiken], Tokyo). In the case of subjects using full dentures, samples were collected from the same regions of the dentures after removal from the oral cavity. From subjects not having any of the above-mentioned teeth, samples were obtained from the opposite teeth. The subjects were asked to chew paraffin gum for 3 min to stimulate secretion of saliva, which was collected into ice-chilled sterile bottles using a cotton swab. Samples from the tonsils were also collected using a cotton swab. All specimens were transferred into 1 ml of reduced transport fluid medium (0.4% agar, 0.15% thioglycollate/phosphate buffered saline) in sterile bottles on ice and processed within one night of collection. The entire samples in tubes were inoculated onto chocolate agar, blood agar, OPA staphylococcus, and drigalski agar plates (Nippon Becton Dickinson Co., Ltd., Tokyo) with an aid of a stick. The plates were incubated in an atmosphere of 5% CO2 in H2 at 37C for 24-48 h. Representative microbial colonies from each plate were gram stained and identified in terms of their characteristic appearance, hemolytic, catalytic reaction, and oxidase reaction (8). Colonies of microbes suspected to be those responsible for pneumonia and which were found in a majority of the subjects were suspended in 1 ml of 0.5% saline and tested by using diagnosis kits indicated below (9). We identified Staphylococcus aureus, both methicillin sensitive (MSSA) and resistant (MRSA) strains, by using PS latex, rabbit plasma, and MRSA screening plates (Nippon Becton Dickinson); Pseudomonas sp. by using VITEK (BioMerieux Vitek Japan [BVJ], Tokyo); b-hemolytic streptococcus by using a Seroidenstrepto kit (Eiken), API strepto (BVJ), and VITEK; Streptococcus pneumoniae by using a Streptococcus identification disk (Nippon Becton Dickinson); Haemophilus influenzae by using a Haemophilus ID4 plate (Nippon Becton Dickinson); Serratia marcescens by using VITEK; and Candida sp. by using Candida check (Iatron Laboratories Inc., Tokyo).
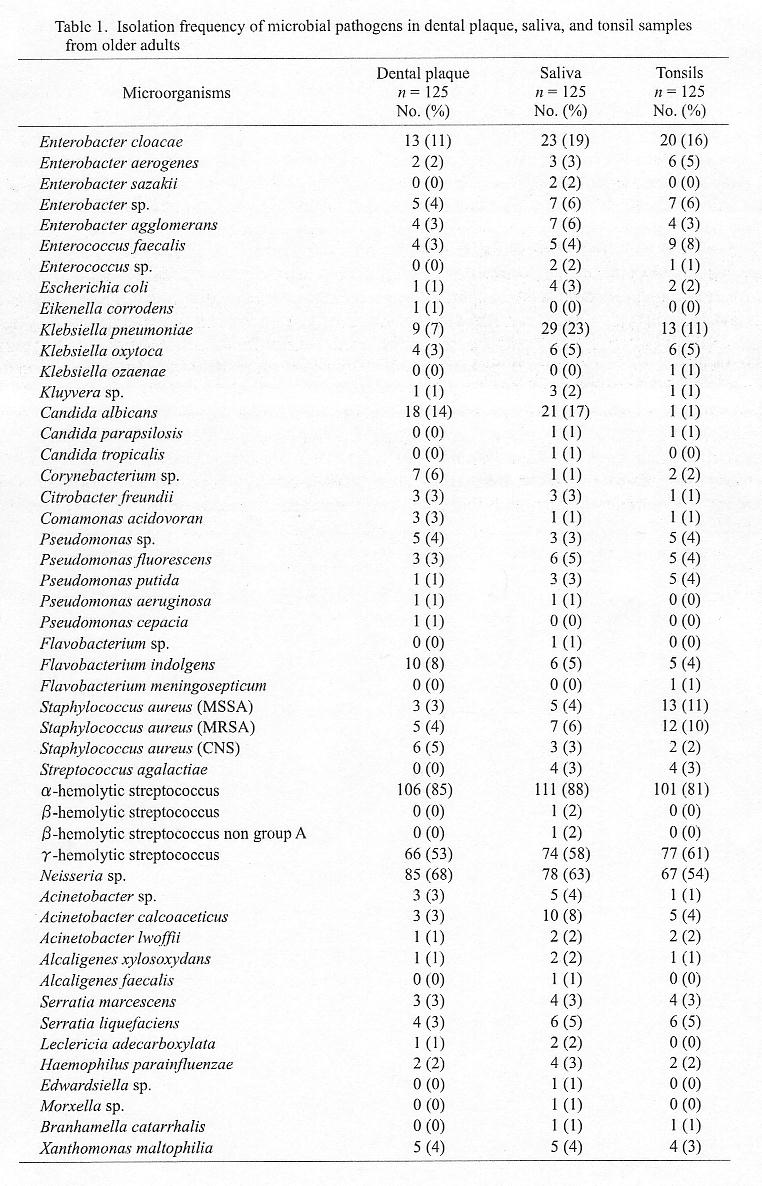
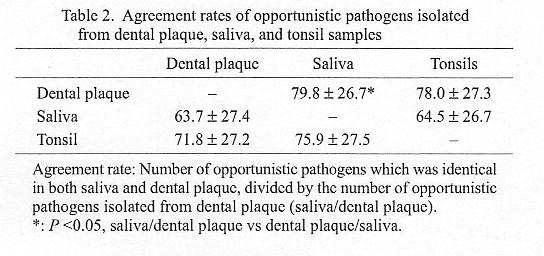
The isolation frequencies of microorganisms from retrieved from dental plaque, saliva, and tonsils, as determined using the manufacturers' instruction, are shown in Table 1. C. albicans, Enterobacteriaceae, Pseudomonas sp., S. areus, Xanthomonas maltophilia, Klebsiella pneumoniae, S. marcescens, coagulase-negative staphylococci (CNS), and K. oxytoca were most frequently isolated from these specimens. The higher prevalence of these microorganisms in elderly subjects indicates that this age population is at greater risk of developing systemic diseases such as pneumonia and heart disease (6). Near 80% of the opportunistic pathogens isolated from dental plaque were found in saliva or tonsils, while 63-64% of the microbes present in saliva were present in dental plaques or tonsils (Table 2). This may indicate that these organisms might be released from tooth surfaces into saliva and then colonize on oral cavity surfaces such as the tonsils. Professional oral hygiene to remove pathogens from dental biofilm may significantly reduce the risk of systemic diseases in elderly people.
REFERENCES
*Corresponding author: Tel: +81-3-5285-1111, Fax: +81-3-5285-1172, E-mail: hsenpuku@nih.go.jp
Go to JJID Homepage Go to JJID 54 (5) Contents
{kind=link}
{kind=link}