Jpn. J. Infect. Dis., 54, 240-242, 2001
To see an article, click this [PDF] link.
Laboratory and Epidemiology Communications
Molecular Epidemiology of Methicillin-Resistant Staphylococcus aureus in a Tokyo Hospital in 2001
Tomoko Fujino, Namiko Mori, Akihiko Kawana, Yoshikazu Naiki, Hisashi Kawahata, Tadatoshi Kuratsuji, Koichiro Kudo, Oichirou Kobori, Yoshio Yazaki and Teruo Kirikae*
International Medical Center of Japan, Toyama 1-23-1, Shinjuku-ku, Tokyo 162-8655
Communicated by Hiroshi Yoshikura
(Accepted December 12, 2001)
Methicillin-resistant Staphylococcus aureus (MRSA) is a major nosocomial pathogen in healthcare facilities (1). Epidemiological analysis of MRSA by means of restriction fragment length polymorphisms of genomic DNA as revealed by pulsed-field gel electrophoresis (PFGE) is essential for assessment of hospital infection controls (2).
Two hundred MRSA isolates were obtained from 61 inpatients in October 2001 in a hospital with 27 wards and 925 beds in Tokyo. Sixty-one of the isolates, each derived from a single patient, were analyzed for chromosomal DNA typing by using a contour-clamped homogeneous electric field system (CHEF MapperTM: Bio-Rad Laboratories, Hercules, Calif., USA), and for antibiotic resistance (WalkAwayTM: Dade Behring, Greefield, Ill., USA), enterotoxin serotyping (SET-RPLA: Denka Seiken Co., Tokyo), toxic shock syndrome toxin-1 (TSST-1) production (TST-RPLA: Denka Seiken), and coagulase serotyping (Denka Seiken). Isolates showing the same PFGE patterns were probably of the same origin.
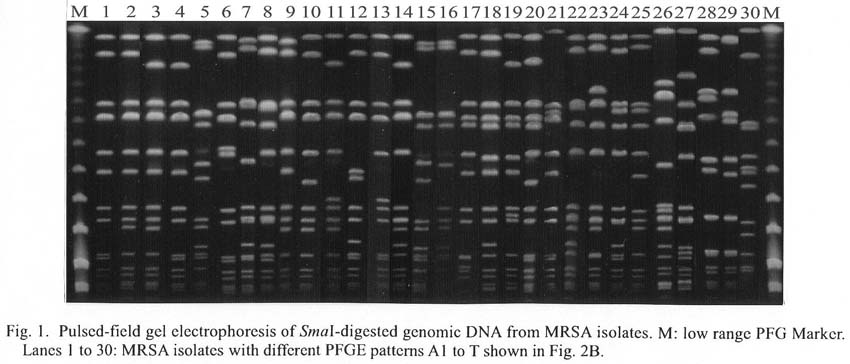
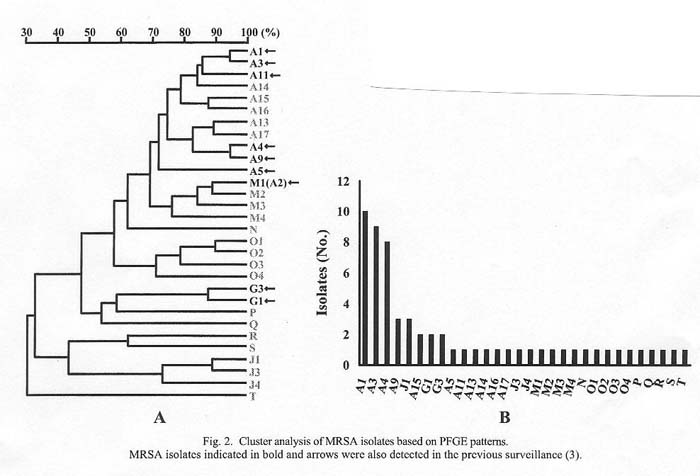
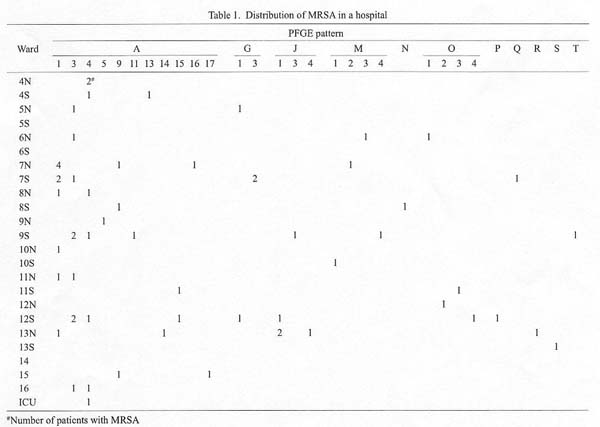
Thirty different PFGE patterns of SmaI DNA digests were detected (Fig. 1). A band-based cluster analysis (Molecular AnalystTM: Bio-Rad), in which PFGE-band similarity exceeding 70% was used as the criterion of cluster formation, revealed 11 pattern clusters: A, G, J, M, N, O, P, Q, R, S, and T (Fig. 2A). Frequency distribution of MRSA of these different PFGE patterns is shown in Fig. 2B. The most frequent pattern (A1), the second most frequent one (A3), and the third most frequent one (A4) represented 15%, 14%, and 12% of total isolates, respectively. Distribution of MRSA isolates in the wards is shown in Table 1. The isolates belonging to PFGE pattern A spread over the different wards; more specifically, PFGE pattern A4 was detected in wards 4N, 4S, 8N, 9S, 12S, 16, and ICU. Two or more different PFGE patterns were detected in some of the same wards, such as 7N, 7S, 9S, 12S, and 13N. The isolates with pattern J1 contributed to a MRSA outbreak in a tuberculosis ward in June 2001 (3).
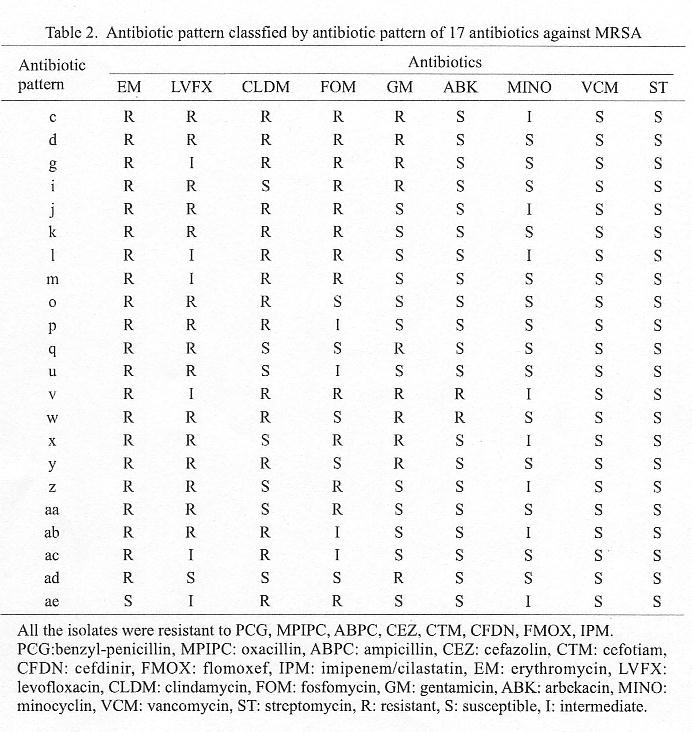
Sensitivity to antibiotics is shown in Table 2. The MRSA isolates had a wide spectrum of drug-resistance; there were 22 different patterns. Those isolates were resistant to 10-13 drugs of the 17 drugs tested. All isolates were sensitive to vancomycin and streptomycin. All of the three isolates with antibiotic pattern u had PFGE pattern J1. No other correlation was found between antibiotic resistance patterns and PFGE patterns (data not shown).
Among the 61 MRSA isolates, 58 isolates produced coagulase type II, and the remaining three produced coagulase type I, III, or IV. Forty-seven isolates produced enterotoxin type C, four isolates enterotoxin type B, three isolates enterotoxin types B and D, two isolates enterotoxin A, one isolate enterotoxin types A and C, one isolate enterotoxin types B and C, and three isolates enterotoxin other than types A, B, C, or D. Forty-nine isolates produced TSST-1, and the other 12 did not. Collectively, among 61 MRSA isolates, 47 isolates produced coagulase type II, enterotoxin type C, and TSST-1.
PFGE-based MRSA surveillance was conducted in the same hospital in December 2000. PFGE patterns A1, A2(M1), A3, A4, A5, A11, G1, and G3 were detected in the present study and in that conducted in December 2000. PFGE patterns A14 to 17, M2 to 4, N, O1 to 4, P, Q, R, S, J1, J3, J4, and T were newly detected the present study. Rapid turnover of MRSA as well as persistence of some other MRSA strains occurred in the hospital.
Phenotyping based on antibiotic sensitivities and other biological properties was found unsuitable for assessing MRSA epidemiology in healthcare facilities.
REFERENCES
*Corresponding author: Fax: +81-3-3202-7364, E-mail: tkirikae@ri.imcj.go.jp
Go to JJID Homepage Go to JJID 54 (6) Contents
{kind=link}
{kind=link}
{kind=link}
{kind=link}