Jpn. J. Infect. Dis., 54, 243-244, 2001
To see an article, click this [PDF] link.
Laboratory and Epidemiology Communications
A Case of Leptospirosis Probably Caused by Drinking Contaminated Well-Water after an Earthquake
Tomohiro Aoki*, Nobuo Koizumi1 and Haruo Watanabe1
Department of Internal Medicine, Nichinan Municipal Hospital, Syoyama 511-7, Nichinan-cho, Hinogun, Tottori 689-5211 and 1Department of Bacteriology, National Institute of Infectious Diseases, Toyama 1-23-1, Shinjuku-ku, Tokyo 162-8640
Communicated by Haruo Watanabe
(Accepted December 18, 2001)
Leptospirosis, a zoonotic disease caused by infection with pathogenic Leptospira, is prevalent in developing countries of the world, especially in Asia and Central and South America (1), though rare in Japan. We here report a recent case of leptospirosis in Japan, in which the subject was probably infected by drinking contaminated well-water after an earthquake.
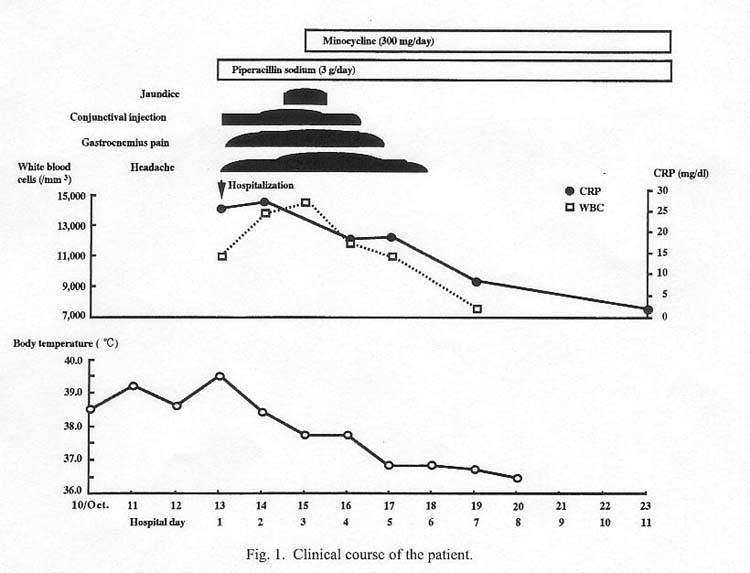
A 48-year-old man had a history of drinking water from a slightly muddy well after an earthquake in the Tottori area on 6 October 2000. He had a fever of 38Åé on 10 October; his condition worsened, accompanied by chills, fatigue, and myalgia. He was admitted to a hospital on 13 October. His body temperature was 39.5Åé, and his heart rate 92/min. Blood pressure was normal. He had a conjunctival injection but no other abnormal findings. White blood cell count was 11,000/ml with 88% segmented neutrophils. Hemoglobin was 14.9 g/dl, platelet count 47,000/ml, total bilirubin 0.8 mg/dl, aspartate aminotransferase (AST) 39 IU/dl, alanine aminotransferase (ALT) 26 IU/dl, lactate dehydrogenase (LDH) 176 IU/dl, blood urea nitrogen (BUN) 12.8 mg/dl, creatinine 0.69 mg/dl, C-reactive protein (CRP) 26 mg/dl, and hematuria (+) and proteinuria positive. The laboratory findings, indicative of inflammation and thrombocytopenia, suggested a severe infection. Cultures of sputum, blood, and urine were negative. Piperacillin sodium (3 g/day) was initially prescribed. On hospital day 3, however, conjunctival injection, headache, and gastrocnemius pain were aggravated and jaundice became prominent. At this point, leptospirosis was suspected, and minocycline (300 mg/day) was given. On hospital day 5, fever dropped to 37Åé and the patient was discharged from the hospital on 21 November 2000 (Fig.1).
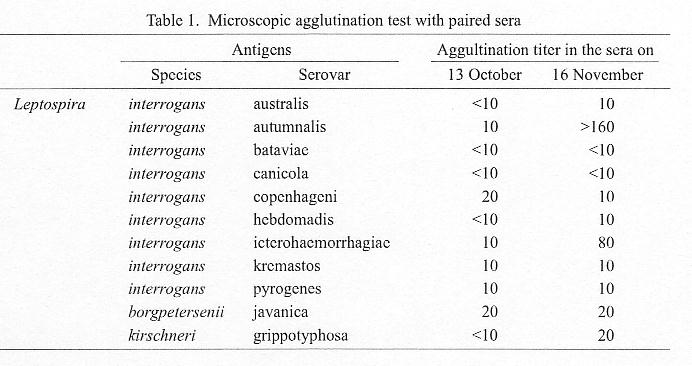
Sera taken on 13 October and 16 November were examined for sero-diagnosis of Leptospira infection by microscopic agglutination (2). Titer of antibody against L. interrogans serovar autumnalis in the serum of 16 November was 16-fold higher than that of 13 October (Table 1).
Incidence of leptospirosis has dramatically decreased in Japan, and yearly reported cases are few. Leptospirosis in our case was probably caused by drinking contaminated well-water after an earthquake. Natural disasters may cause contamination of drinking water by rat urine containing Leptospira. In tropical regions, outbreaks of leptospirosis often occur after heavy rain and flood (1). Our recent investigations revealed the presence of leptospires in urine of rats trapped in urban areas (unpublished data). The possibility of leptospirosis should not be ignored when physicians see patients with fever of unknown origin after natural disasters.
This article appeared in the Infectious Agents Surveillance Report, vol.22, No.7, p.7, 2001 in Japanese.
REFERENCES
Go to JJID Homepage Go to JJID 54 (6) Contents
{kind=link}
{kind=link}