Jpn. J. Infect. Dis., 55, 29-30, 2002
To see an article, click this [PDF] link.
Laboratory and Epidemiology Communications
Molecular Epidemiology of Methicillin-Resistant Staphylococcus aureus in a Kumamoto Hospital in 2001
Fumio Kawano*, Hisayoshi Miyazaki, Jun-ichi Takami, Tomoko Fujino1, Katsutoshi Saruta1 and Teruo Kirikae1
Kumamoto National Hospital, Ninomaru 1-5, Kumamoto 860-0008 and 1International Medical Center of Japan, Toyama 1-21-1, Shinjuku-ku, Tokyo 162-8655
Communicated by Hiroshi Yoshikura
(Accepted April 3, 2002)
Methicillin-resistant Staphylococcus aureus (MRSA) is a major nosocomial pathogen in healthcare facilities (1). Epidemiological analysis of MRSA isolates present in a hospital, assisted such as by restriction fragment length polymorphisms of genomic DNA using pulsed-field gel electrophoresis (PFGE), is essential for assessment of hospital infection controls (2).
Fifty-six MRSA isolates were obtained from 22 inpatients from October 2001 in a hospital with 11 wards and 550 beds in Kumamoto Prefecture. Among these isolates, 22 isolates, each derived from a single patient, were analyzed for chromosomal DNA typing by using a contour-clamped homogeneous electric field system (CHEF MapperTM: Bio-Rad Laboratories, Hercules, Calif., USA), antibiotic resistance (VITEKTM: bioMerieux, Marcy-l'Etoile, France), enterotoxin serotyping (SET-RPLA: Denka Seiken Co., Tokyo), toxic shock syndrome toxin-1 (TSST-1) production (TST-RPLA: Denka Seiken), and coagulase serotyping (Denka Seiken). In the present study, the isolates showing the same PFGE patterns were considered to have the same origin.
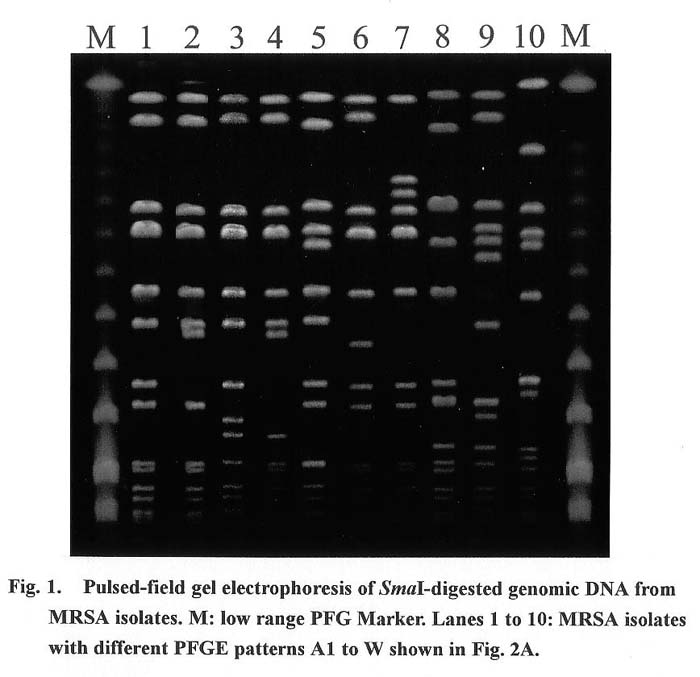
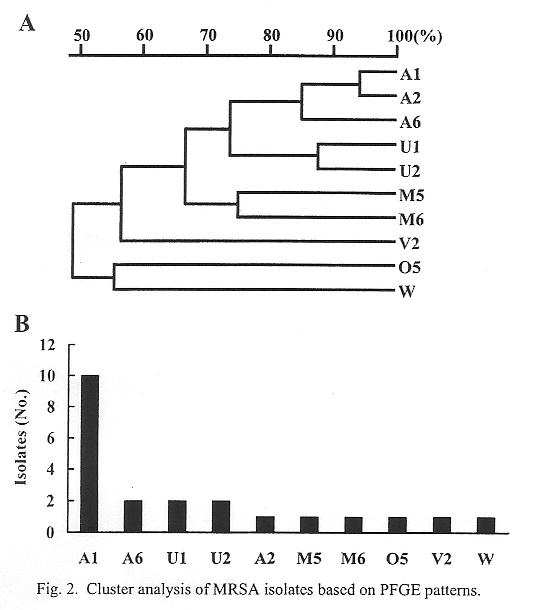
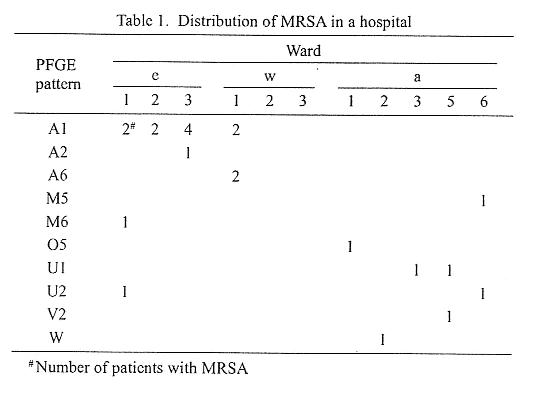
Ten different PFGE patterns of SmaI DNA digests were detected (Fig. 1). A band-based cluster analysis of these patterns (Molecular AnalystTM: Bio-Rad) revealed five clusters (clusters A/U, M, V, O, and W) (a cluster was defined as a group of patterns with more than 70% similarity) (Fig. 2A). A frequency distribution of MRSA isolates based on PFGE patterns is shown in Fig. 2B. The most frequent pattern (A1) represented 45.5% of the total isolates. The top five clusters, A1, A6, U1, U2, and A2, made up 77.3 % of the total isolates. A geographic distribution of MRSA isolates in the hospital is shown in Table 1. The two, two, four, and two isolates from wards e1, e2, e3, and w1, respectively, belonged to the same cluster, A1, suggesting a quite extensive spread by secondary infections. Moderate spread was observed for MRSA in cluster groups U1 and U2, i.e., two isolates from wards a3 and a5 belonged to the same cluster, U1, and two isolates from wards e1 and a6 to the same cluster, U2. Two isolates belonging to cluster A6 were isolated from the ward w1, suggesting a spread within the ward. Isolates with patterns A2, M5, M6, O5, V2, and W appeared to be limited to wards e3, a6, e1, a1, a5, and a2, respectively.
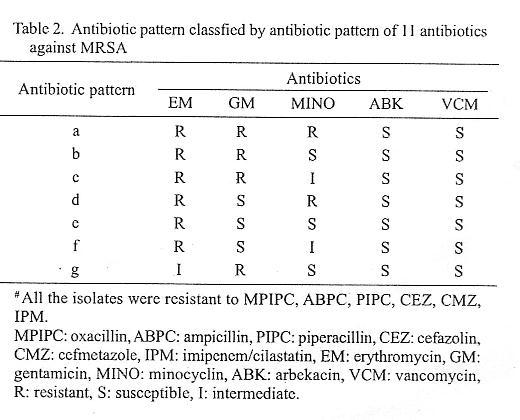
Sensitivity to antibiotics is shown in Table 2. The MRSA isolates had a spectrum of drug-resistance showing seven different patterns. Those isolates were resistant to 7 - 9 of 11 tested drugs. No isolate was resistant to either vancomycin or arbekacin. No correlation was found between the antibiotic patterns and PFGE patterns (data not shown).
Among 29 MRSA isolates, 27 isolates produced coagulase type II, and two isolates produced coagulase typeÅE. Twenty-six isolates produced enterotoxin type C, three isolates enterotoxin type B, three isoletes enterotoxin types B and D, and three isolates enterotoxin other than types A, B, C, and D. Twenty-six isolates produced TSST-1, but three did not produce it. Collectively, among 29 MRSA isolates, 26 isolates produced coagulase type II, enterotoxin type C, and TSST-1, i.e., most of the isolates shared common characteristics regarding these parameters.
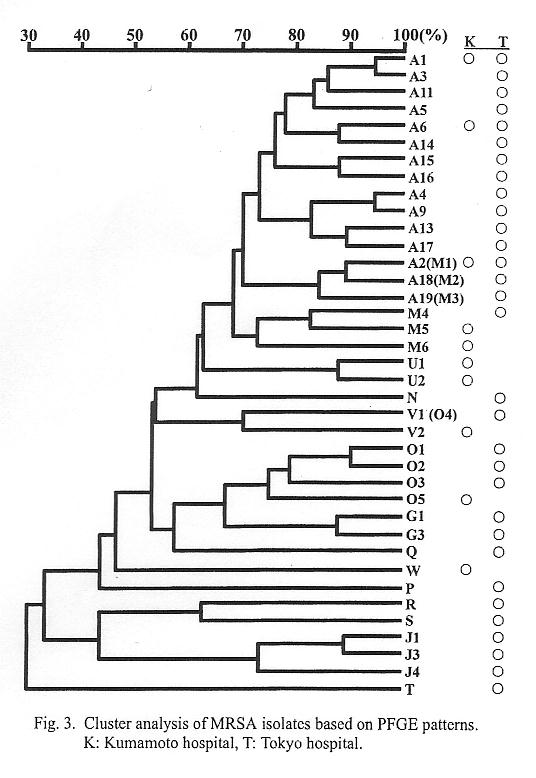
Patterns A1, A6, and A2 (M1) detected in this hospital had been detected in a hospital in Tokyo (Fig. 3)(2,3). Among these patterns, pattern A1 was the most frequent in both hospitals (Fig. 2B)(2,3). The data indicate the clonal expansion of MRSA not only within hospitals but also nationwide.
REFERENCES
*Corresponding author: Fax: +81-96-325-2519, E-mail: f-kawano@sa2.so-net.ne.jp
Go to JJID Homepage Go to JJID 55(1) Contents
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}