Jpn. J. Infect. Dis., 55, 58-59, 2002
To see an article, click this [PDF] link.
Laboratory and Epidemiological Communications
Antimicrobial Resistance Pattern of Salmonella typhi Isolates in Kolkata, India during 1991-2001: a Retrospective Study
Shyamapada Mandal*, Manisha Deb Mandal and Nishith Kumar Pal
Department of Bacteriology and Serology, Calcutta School of Tropical Medicine, C.R. Avenue, Kolkata-700073, India
Communicated by Haruo Watanabe
(Accepted May 29, 2002)
Typhoid fever remains a serious problem in India due to the emergence of multidrug resistant Salmonella typhi, which has been reported since 1983 (1). The strain showed resistance to ampicillin (A), chloramphenicol (C) and cotrimoxazole (Co), the conventional antityphoid antibiotics. Despite resistance to A, C, and Co, S. typhi is susceptible to ciprofloxacin, which has replaced A, C, and Co in the empirical treatment of typhoid fever (2), and thus has resulted in the reemergence of S. typhi isolates sensitive to A, C, and Co due to the withdrawal of selection pressure (3). But unrestricted use of the conventional antibiotics has led to the emergence of multidrug resistant S. typhi isolates again in very recent years (4). We isolated a total number of 421 S. typhi isolates from blood samples of enteric fever patients during 1991 to 2001. The aim of the present study was to asses the changing trends of antibiotic susceptibility pattern among S. typhi isolates in and around Kolkata, India.
A total of 421 S. typhi isolates were tested for antibiotic susceptibility pattern by the agar dilution method (5) using Mueller-Hinton agar medium against A, C, Co, and tetracycline (T). The amount of antimicrobial agents (mg/ml) were A (25), C (30), Co (25), and T (10). Escherichia coli ATCC 25922 strain was used as control. The S. typhi isolates used in the study were obtained from the blood of patients clinically suspected of enteric fever who attended the Calcutta School of Tropical Medicine from January 1991 to December 2001.
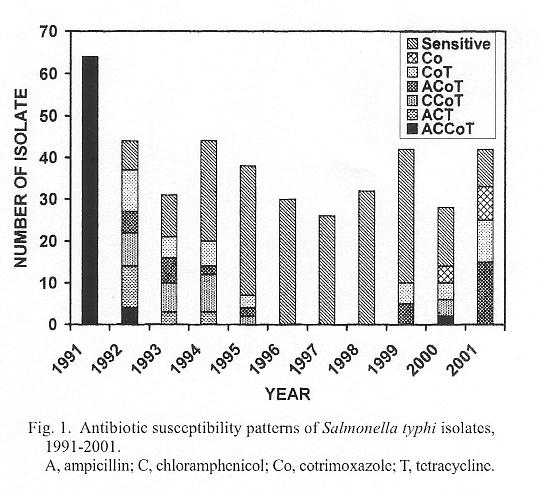
The antibiotic susceptibility patterns of 421 S. typhi isolates obtained from 1991 to 2001 are shown in Figure 1. In 1991, all 64 (100%) isolates showed a pattern of resistance to ACCoT. In following 4 years (1992-1995) various resistance patterns were found: ACCoT, ACT, CCoT, AcoT, and CoT along with the emergence of antibiotic sensitive isolates in an increasing manner (15-82%). From 1996 to 1998, the isolates showed 100% sensitivity to A, C, Co, and T. During last 3 years (1999-2001) of the study period, a decrease in frequency of sensitive isolates (76-21%) and reemergence of resistant isolates showing patterns of resistance to ACCoT, ACoT, CCoT, CoT, and Co were noticed. Changing patterns of antibiotic resistance of S. typhi have been reported earlier (3,4). Thus our data suggest that constant surveillance for antibiotic susceptibility patterns of current S. typhi isolates is imperative for determining effective treatment policies.
REFERENCES
*Corresponding author: E-mail: samtropmed@rediffmail.com
Go to JJID Homepage Go to JJID 55 (2) Contents
{kind=link}