Jpn. J. Infect. Dis., 55, 62-65, 2002
To see an article, click this [PDF] link.
Laboratory and Epidemiology Communications
Discordant Movement of CD4-Positive T-Cell Count in HIV-1 Infected Patients with HAART Failure
Aiko Okano, Masakazu Matsuda, Tomoko Chiba, Kenji Moriya, Kaneo Yamada1 and Wataru Sugiura*
AIDS Research Center, National Institute of Infectious Diseases, Gakuen 4-7-1, Musashimurayama, Tokyo 208-0011 and 1St. Marianna University School of Medicine, Sugao 2-16-1, Miyamae-ku, Kawasaki, Kanagawa 216-8511
Communicated by Naoki Yamamoto
(Accepted June 7, 2002)
Highly active antiretroviral treatment (HAART) with at least one protease inhibitor (PI) and two nucleoside reverse transcriptase inhibitors (NRTIs) is now the recommended first-line antiretroviral prescription for HIV-1 infection (1,2). While its introduction has greatly improved the prognoses of many of patients (3-5), HAART has been unsuccessful in a considerable number of cases (6,7). This treatment failure is due mainly to the emergence of drug resistant HIV-1. Once the drug resistant virus appears, it will quickly predominate in the virus population due to selective advantage under continued drug administration. Insufficient suppression of virus replication, gradual decrease of peripheral CD4+ T-cell count, and consequent accelerated disease progression are frequent outcomes (8-10). Recently, however, several groups have reported cases in which the rise and fall of CD4+ T-cell counts and viral copy numbers during HAART did not follow the rule above (11,12).
We examined 236 HIV-1 infected patients who had been treated in 17 hospitals collaborating with our laboratory and followed up for more than 4 years (from November 1996 to September 2000).
CD4+ T-cell count and clinical data were provided by the collaborating hospitals. Viral load (VL) was measured by using AMPLOCOR HIV-1 MONITORTM Test Version 1.5 (Roche Diagnostics, Branchburg, N.J., USA).
HIV-1 pol sequences were analyzed for drug resistance genotypes. RNA was extracted form 200 mL of plasma by using an RNA purification kit (Boehringer Mannheim, Indianapolis, Ind., USA), and the 821 bp reverse transcriptase (RT) and 380 bp protease (PR) regions were reverse transcribed and amplified by nested PCR in a previously reported manner (13). The amplified fragments were directly sequenced using dye-terminator chemistry (14) and the auto-sequencer ABI-377 (Applied Biosystems, Foster City, Calif., USA).
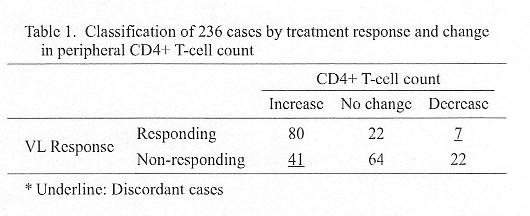
The 236 cases were classified according to their VL response and changes in CD4+ T-cell count (Table 1). VL responses were classified into two groups, either (i) responding: VL achieved below the detectable level (<50 copies/mL) or >2 log copies/mL of reduction from the baseline before treatment, or (ii) non-responding: not applicable to category (i). Each VL response class was categorized into three according to CD4+ T-cell counts: (a) increase: absolute increase from the baseline before treatment, (b) decrease: absolute decrease from the baseline before treatment, (c) no change: no significant increase or decrease during the observation period.
As summarized in Table 1, in the VL responding group (n = 109), the number of cases applicable to categories (a), (b), and (c) were 80, 22, and 7, respectively. In the VL non-responding group (n = 127), the number of cases applicable to (a), (b), and (c) were 41, 64, and 22 cases, respectively. Thus, the responding group had a significantly high number of category (a), i.e., cases with increased CD4+ T-cell count, (P < 0.001). In contrast, the non-responding group had significantly high numbers of categories (b) + (c), cases whose CD4+ T-cell did not increase during the therapy (P < 0.001). As has been previously reported, and found as well in our samples, some cases have shown discordance between VL response and CD4+ T-cell response. Forty-one VL non-responding cases demonstrated increased CD4+ T-cell count, and seven VL responding cases showed a decrease in CD4+ T-cell count.
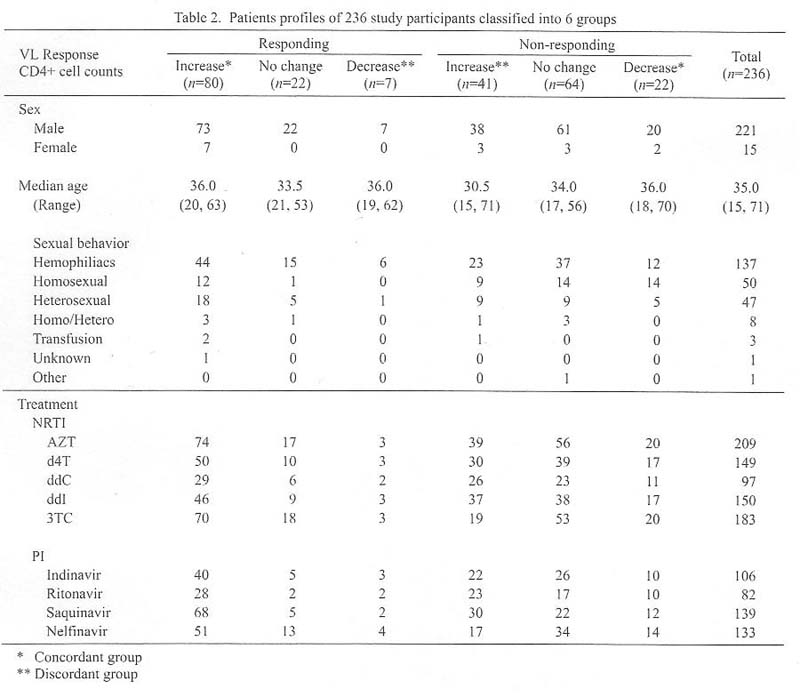
Patient profiles of each category are summarized in Table 2. No significant difference was seen in regard to sex, sexual behaviors and treatment protocols. Only parameter in which a significant difference could be seen was the lower median age, 30.5 years, of the patients with "VL non-responding-CD4+ increase", i.e., (ii) (a) cases.
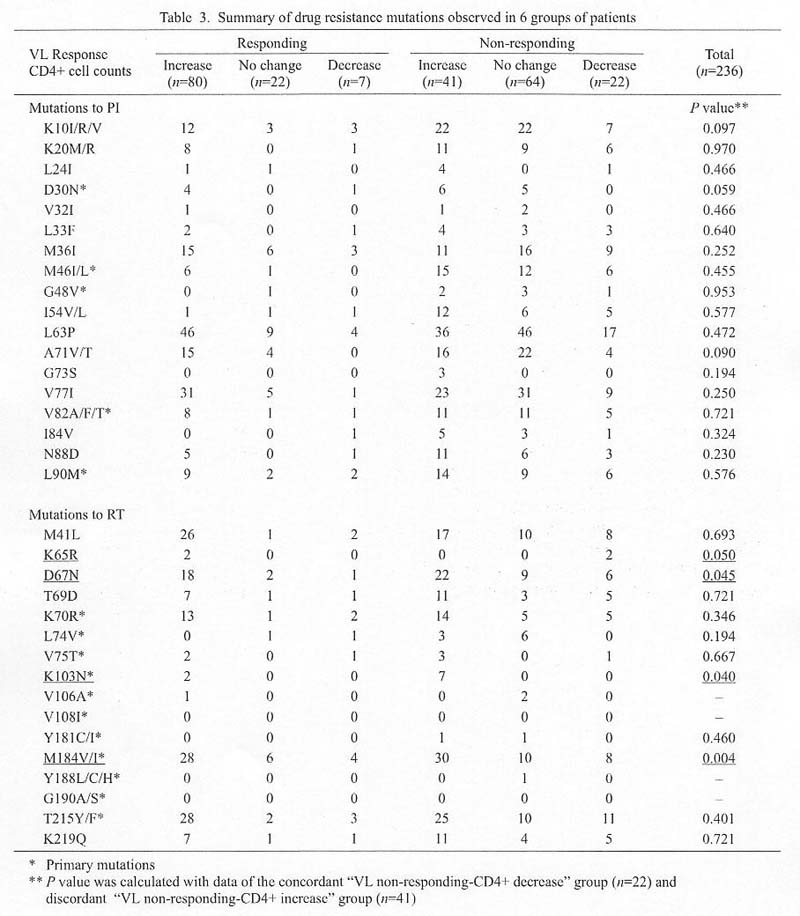
In the drug resistance genotype comparison (Table 3), the incidence of D67N, K103N, and M184V/I RT-related resistance mutations was significantly higher in the discordant "VL non-responding-CD4+ increase" group (n = 41) than in the concordant "VL non-responding-CD4+ decrease" group (n = 22) (P = 0.045, 0.040, and 0.004, respectively). Regarding protease inhibitor-resistant mutations, no significant association could be seen between mutations and the discordance pattern.
Our results confirmed that virologic failure did not always result in acute immunologic failure. The cause of this discordance remains unclear, necessitating further research. The further study might help answer fundamental questions regarding HIV-1 pathogenesis and may provide clues to the proper timing for changing antiretroviral regimens after virologic failure.
REFERENCES
*Corresponding author: Fax: +81- 42-561-7746, E-mail: wsugiura@nih.go.jp
Go to JJID Homepage Go to JJID 55 (2) Contents
{kind=link}
{kind=link}
{kind=link}