Jpn. J. Infect. Dis., 55, 93-95, 2002
Laboratory and Epidemiology Communications
Molecular Epidemiological Surveillance of Methicillin-Resistant Staphylococcus aureus in a Hiroshima Community Hospital in 2002
Rie Sasaki, Tomoko Fujino1, Katsutoshi Saruta1, Junko Kawasaki, Norikazu Shigeto and Teruo Kirikae1*
Hiroshima City Medical Association-Administered Aki City Hospital (former National Hataka Hospital), Hataka 2-14-1, Aki, Hiroshima 736-0088 and 1International Medical Center of Japan, Toyama 1-21-1, Shinjuku-ku, Tokyo 162-8655
Communicated by Hiroshi Yoshikura
(Accepted July 10, 2002)
Methicillin-resistant Staphylococcus aureus (MRSA) is a major hospital-acquired pathogen in institutions including community hospitals with relatively small numbers of beds (1,2). Molecular epidemiological surveillance using restriction fragment-length polymorphisms of genomic DNA employing pulsed-field gel electrophoresis (PFGE) is essential for assessment of hospital infection controls (3).
The present surveillance was conducted in a hospital in Hiroshima. The hospital had two wards totaling 120 beds. The subjects included 100 inpatients and 111 medical staff members present in the hospital in February 2002. A total of 39 MRSA isolates were obtained from five patients' sputa, one patient's bedsore, and nasal swabs of ten patients and three nurses in ward I; five patients' sputa, two patient's urine, nasal swabs of eight patients and three nursing staff members including one nurse and two assistant nurses in ward II; and nasal swabs of one doctor and one nurse in charge of outpatients. Carriage rates of MRSA were 31% for inpatients and 9% for medical staff members. The isolates were tested for chromosomal DNA typing by using a contour-clamped homogeneous electric field system (CHEF MapperTM: Bio-Rad Laboratories, Hercules, Calif., USA), enterotoxin serotyping (SET-RPLA: Denka Seiken Co., Tokyo), toxic shock syndrome toxin-1 (TSST-1) production (TST-RPLA: Denka Seiken), and coagulase serotyping (Denka Seiken).
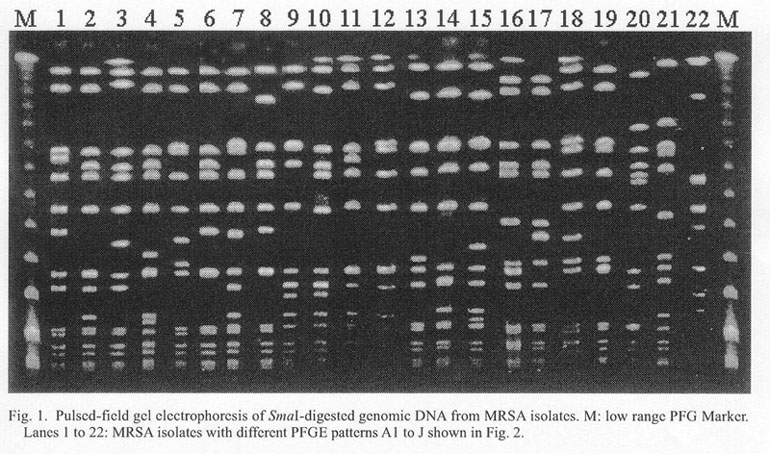
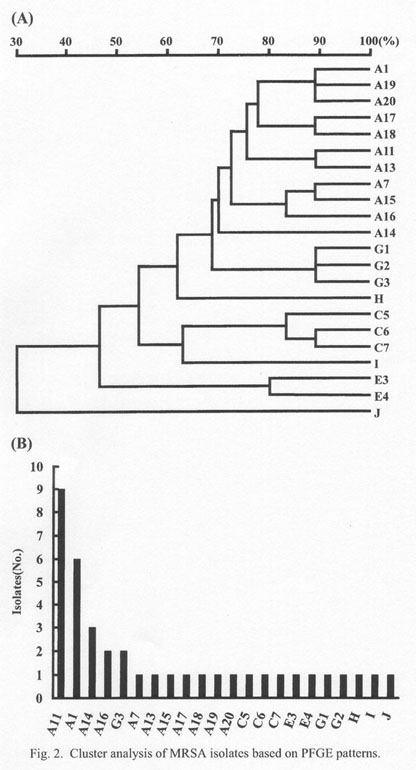
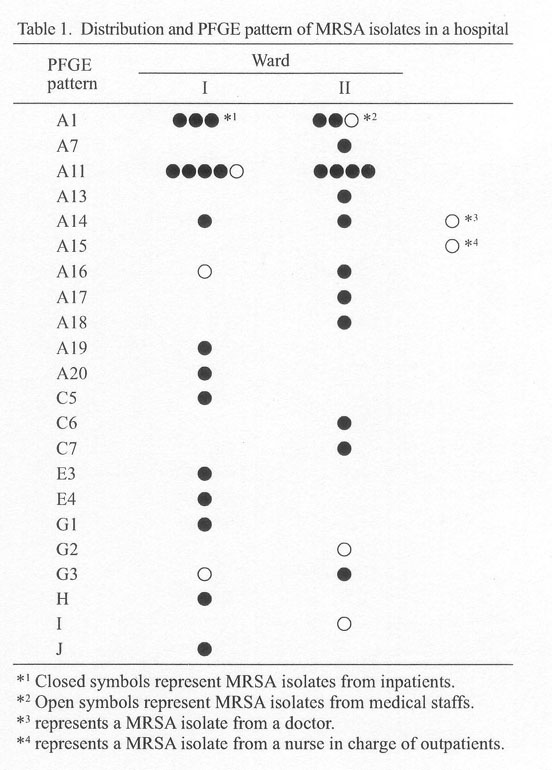
Twenty-two different PFGE patterns of SmaI DNA digests were detected (Fig. 1). A band-based cluster analysis (Molecular AnalystTM: Bio-Rad), in which PFGE-band similarity exceeding 70% was used as the criterion of cluster formation, revealed 7 cluster patterns: A, G, H, C, I, E, and J (Fig. 2A). The frequency distribution of MRSA of these different PFGE patterns is shown in Fig. 2B. The most frequent pattern (A11) and the second-most frequent one (A1) represented 29% and 19% of the total isolates, respectively. Distribution of MRSA isolates in the wards is shown in Table 1. The isolates belonging to PFGE patterns A11 and A1 were the most common and were spread over wards I and II. Three isolates having PFGE pattern A14 were obtained from patients in both wards I and II as well as from a doctor. PFGE patterns A16 and G3 were detected in both wards I and II. The remaining 17 PFGE patterns were detected from a single patient or medical staff member.
Among the 39 MRSA isolates, 37 isolates produced coagulase type II, and the remaining two produced coagulase type I or III. Twenty-five isolates produced enterotoxin type C, two isolates enterotoxin type B, nine isolates enterotoxin types B and C, one isolate enterotoxin A, and one isolate enterotoxin other than types A, B, C, or D. Thirty-four isolates produced TSST-1, while the other five did not. Collectively, among 39 MRSA isolates, 25 isolates produced coagulase type II, enterotoxin type C, and TSST-1. Nine isolates with PFGE pattern A11 produced coagulase type II, enterotoxin types B and C, and TSST-1.
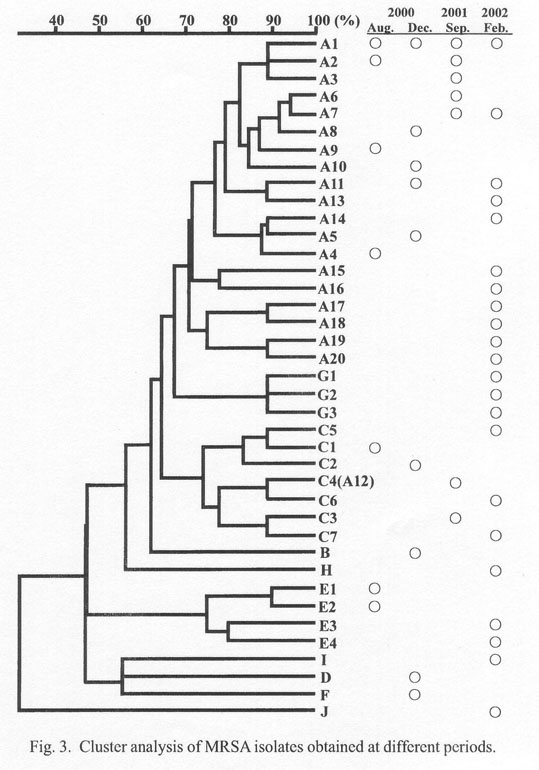
The PFGE patterns of these MRSA isolates were compared with those of MRSA isolates obtained in the same hospital in August and December 2000 (1), and in September 2001 (2). From a total of 70 isolates, 39 different PFGE patterns were detected (data not shown). Band-based cluster analysis of these patterns revealed 10 clusters A to J (Fig. 3). Four of seven PFGE patterns in August 2000, five of nine in December 2000, five of seven in September 2001, and 11 of 22 in February 2002 were of cluster type A. PFGE pattern A1 was detected during all the investigated periods. Pattern A2 was detected in August 2000 and September 2001, pattern A7 was detected in September 2001 and February 2002, and pattern A11 was detected in December 2000 and February 2002. Collectively, the above observations indicate the spread of two MRSA strains with patterns A11 and A1 in the hospital in February 2002. Pattern A1 strain had settled in the hospital before December 2000 and continued to circulate. Another strain with pattern A11 which appeared in December 2000 was a newcomer to the hospital. Other MRSAs whose infections were sporadic were considered to be introduced from outside.
REFERENCES
*Corresponding author: Fax: +81-3-3202-7181, E-mail: tkirikae@ri.imcj.go.jp
Go to JJID Homepage Go to JJID Contents 55 (3)
{kind=link}
{kind=link}
{kind=link}
{kind=link}