Jpn. J. Infect. Dis., 55, 95-97, 2002
Laboratory and Epidemiology Communications
Eradication of poliomyelitis in Ethiopia: Virological and Acute Flaccid Paralysis Surveillance
Berhane Beyene Mentaye*, Oyewale Tomori1, Oywale Femi2, Almaz Gebere Senbet3 and Tilahun Woldemichael4
Polio Laboratory, Ethiopian Health and Nutrition Research Institute, P.O. Box 1242, 2World Health Organization Country Office, P.O. Box 3069, 3Disease Prevention and Control Department, Ministry of Health of Ethiopia, P.O. Box 1242, 4Ethiopian Health and Nutrition Research Institute, P.O. Box 1234, Addis Ababa, Ethiopia and 1World Health Organization Africa Office, P.O. Box BE 773, Harare, Zimbabwe
Communicated by Hiroshi Yoshikura
(Accepted July 17, 2002)
In Ethiopia, as in other Third World countries, poliomyelitis is a major public health problem affecting mainly preschool children (1).
A study conducted at a major pediatric hospital in Addis Ababa demonstrated an increase in new cases between 1971 and 1981. Eighty-nine percent of the cases with residual paralysis were 2-year-old children. There was no seasonal variation. A study in 1979 involving over a quarter of a million school age children in Addis Ababa indicated a prevalence of 2.7/1,000, with an estimated annual incidence of 7.8/100,000 (2). Another study, conducted from February to July in 1993, indicated that the prevalence among children aged 5-9 years was 7.3/1,000 (3). Other school and institutional based studies revealed a higher prevalence (4).
The key to evaluating the status of polio eradication is combining epidemiological and laboratory investigations of acute flaccid paralysis (AFP) among infants and children (5).
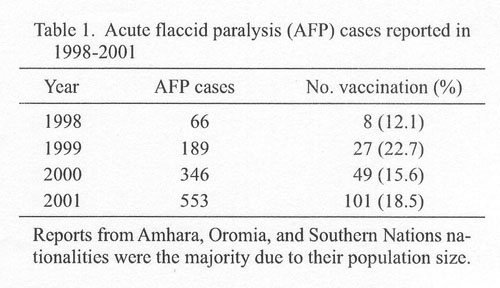
Table 1 shows AFP cases reported in 1998-2001 and vaccination history. One important criterion of proper AFP surveillance is the minimum detection of at least one AFP case among 100,000 children under 15 years of age. Given that the corresponding population is about 30 million in Ethiopia, the number of expected AFP cases is 300.
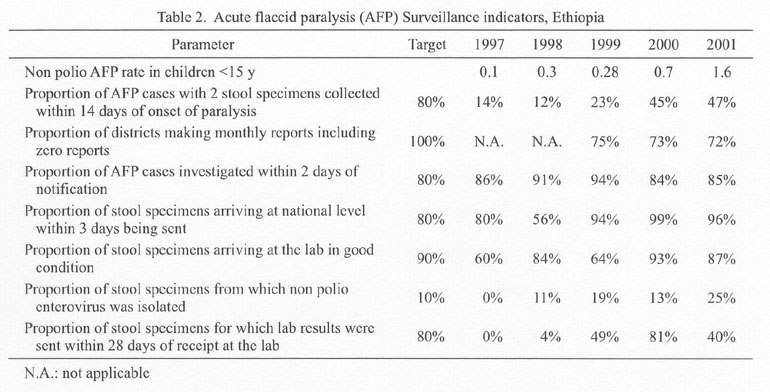
The AFP surveillance indicators are shown in Table 2. From 1997 to 2001, Ethiopia made remarkable progress. However, the rate of collection of two stool specimens within 14 days after onset of paralysis remains unsatisfactorily low.
Table 3 shows the record of specimens sent to National Polio Laboratory, Ethiopian Health and Nutrition Research Institute. In 1997, we received only nine stool specimens in total from the Oromia and Addis Ababa regions. In l998, the stool specimen number increased to 65, owing to improved AFP surveillance. In 2001, we received 1,048 stool specimens derived from 553 AFP cases. The isolates were shipped to Johannesburg Regional Referral Laboratory for intra-typic differentiation by probe hybridization and ELISA.
Table 4 shows a detailed description of five cases from which wild-type polioviruses were isolated. The isolates were all type 1. Three of these patients had not received oral poliovirus vaccine (OPV). Residual paralysis was observed in four of the five patients. DNA sequencing at the Centers for Disease Control and Prevention, Atlanta, Ga., USA, revealed that the wild-type isolates in 1999-2001 were not related to other viruses isolated in neighboring countries or elsewhere. It is unlikely that the virus was imported from outside. The last case was a child in Muda Gerama Kebele in Kedida Gamela Woreda of the Kembata zone (southern part of Ethiopia).
The authors thank Dr.Balcha of the Girma Epidemiology Department; the AFP surveillance officers at WHO; Mr. Tesfaye Bedada, WHO data manager; National Polio Laboratory personnel; and the personnel from the 11 regions and 71 zones in Ethiopia, who are part of the polio surveillance system and provided us with the original surveillance information. The authors would also like to thank the Japanese International Cooperation Agency for support of research conducted in the Polio Laboratory, Ethiopian Health and Nutrition Research Institute, since 2001.
REFERENCES
*Corresponding author: Fax: +251-1-774722, E-mail: Berhane12@yahoo.com
Go to JJID Homepage Go to JJID Contents 55 (3)
{kind=link}
{kind=link}
{kind=link}
{kind=link}