Jpn. J. Infect. Dis., 55, 97-99, 2002
Laboratory and Epidemiology Communications
Evaluation of the School Health Surveillance System for Influenza, Tokyo, 1999-2000
Hayato Fujii1,5*, Hiroshi Takahashi2, Takaaki Ohyama2, Kinuyo Hattori3 and Shigeto Suzuki3,4
1Field Epidemiology Training Program and 2Infectious Disease Surveillance Center, National Institute of Infectious Diseases, Toyama 1-23-1, Shinjuku-ku, Tokyo 162-8640, 3Tokyo Metropolitan Research Laboratory and Public Health, Hyakunin-cho 3-24-1, Shinjuku-ku, Tokyo 169-1173, 4Reimeikai-Minamidai Hospital, Ogawa-machi 1-485, Kodaira-shi, Tokyo 187-0032 and 5Community Medicine Section, Public Health and Welfare Bureau, Kamihonnoujimae-cho 488, Teramachi Oike, Nakagyo-ku, Kyoto 604-8571
Communicated by Kunihiko Masukawa
(Accepted July 23, 2002)
The school health surveillance system (SHSS) is the sole notifiable surveillance system in Japan for indicating the presence of pediatric influenza (1). To measure the magnitude of influenza among schoolchildren in all 47 prefectures, the Ministry of Education, Science, Sports and Culture and the Ministry of Health, Labour and Welfare have jointly run the SHSS since the school health law was enacted in 1958. Here, the schools are asked to report number of absentees with influenza-like illness (ILI) when it had school/class closure. Principal of the school can decide the closure, usually for 2-4 days, if absentees reached above 20% of students.
By comparing the SHSS data with the national sentinel surveillance system for influenza (ISSS) data, we found that the SHSS had levels of sensitivity, specificity, and predictive value positive (PVP) comparable to those of the ISSS (2). However, as this study was based upon only the national sentinel surveillance data during the 2nd through 11th week of 1998 and 1999 for all prefectures in Japan, trends in specific regions in Japan under a longer time frame could not be assessed.
In the present analysis, SHSS and ISSS data were compared for the age group 4 -14 years during the 49th week of 1999 through the 13th week of 2000 (except for winter vacation from 52nd of 1999 to 1st week of 2000). Tokyo had 36 pediatric sentinel sites reporting influenza cases weekly on a regular basis. Ten percent of the patients in such sites were regularly checked for influenza virus in their throat lavage (virological testing done by the Tokyo Metropolitan Research Laboratory and Public Health, Tokyo).
Gargle and blood specimens were also collected from schoolchildren with ILI during the study period. We used the gargled water for virus isolation in Madin-Darby canine kidney (MDCK) cells and identification by specific neutralizing anti-influenza ferret sera (provided by the National Institute of Infectious Diseases, Tokyo). Virus, once isolated from gargled water, was subjected to reverse transcriptase polymerase chain reaction (RT-PCR) in order to detect the virus genome. Virus diagnosis was done by either neutralization or RT-PCR or by the both. For paired blood specimens of absentee children, we performed the complement fixation test to determine if antibody titer increased over fourfold, which we judged as positive.
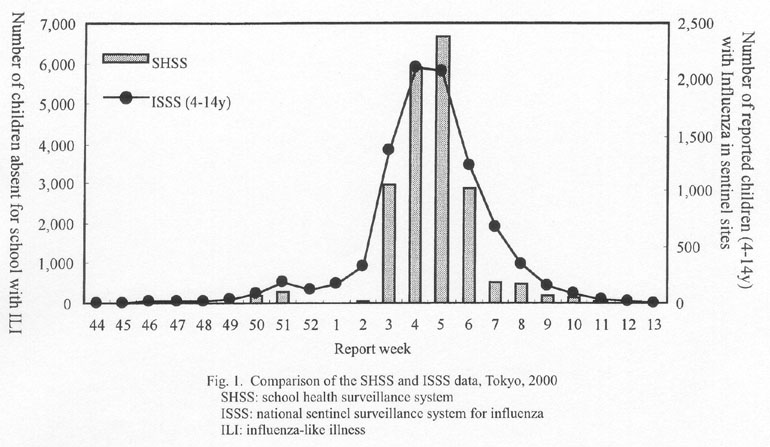
Figure 1 compares the SHSS and the ISSS data during the observation period. Similar trends were observed for SHSS and ISSS. The epidemic status was observed from the 3rd week through the 6th week of the new year.
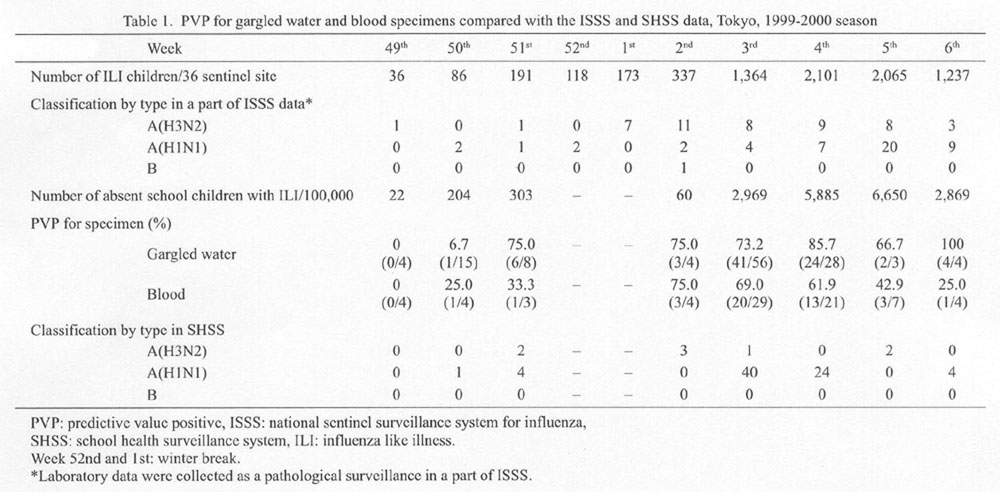
The PVP data for the gargle and blood specimens are shown in Table 1. The acceptable PVP for the gargle specimens was obtained during the 51st week in the previous year through the 6th week of the new year. The acceptable PVP was obtained only on the 2nd and 3rd weeks for the blood specimens.
According to the report by the Tokyo Metropolitan Research Laboratory and Public Health (3), the magnitude of influenza epidemic was rather larger than usual in Tokyo in the 1999/2000 season. The average of the cumulative number of influenza patients per sentinel site in 1999/2000 was over 20. There was a peak in the 3rd - 5th weeks as usual. A major epidemic of influenza type A was seen. The ratio H1N1: H3N2 was 2.4:1 in the 4-15 age group, and the ratio was 1:3 in those aged over 16. Peaks of H3N2 and H1N1 were observed in 5th and 4th - 7th weeks, respectively.
Of a total of 81 influenza virus-positive gargle specimens (either by isolation or RT-PCR), 73 (90.1%) were type A (H1N1), and 8 (9.9%) type A (H3N2). No other type was detected. Of 50 virus isolation-positive gargle specimens, 42 (84%) were type A (H1N1), and 8 (16%) type A (H3N2).
Influenza consistently occurs among school-aged children, followed by spread among family members (4). Both the SHSS and ISSS data showed a consistent rise from the 49th week. As the observed populations in both systems are from the same age group, the majority of ILI patients in both SHSS and ISSS are absentees in class closures. This suggests that the epidemic trend among school-aged children can be easily assessed by SHSS alone (without requiring ISSS).
This study was planned and developed under support of a Japanese Ministry of Health, Labour and Welfare scientific research grant on "coordination for the national and prefectural surveillance systems" (H13-Shinko-5).
REFERENCES
*Corresponding author: Tel: +81-75-222-3421, Fax: +81-75-222-3416, E-mail: fujiih@jmail.plala.or.jp
Go to JJID Homepage Go to JJID Contents 55 (3)
{kind=link}
{kind=link}