Infectious Deseases
Basic Research
Surveillance
Information
- Details
Published: October 26, 2022
Center for Field Epidemic Intelligence, Research and Professional Development,
National Institute of Infectious Diseases
Center for Surveillance, Immunization, and Epidemiologic Research,
National Institute of Infectious Diseases
We would like to express our deepest condolences to the bereaved families of all those who have passed away after SARS-CoV-2 infection.
Background and objectives
The Ministry of Health, Labour, and Welfare (MHLW) requested local public health authorities to conduct genome analysis of severe and fatal cases of SARS-CoV-2 infection to accumulate and monitor knowledge on the severity of SARS-CoV-2 infection on the basis of “the enhanced field epidemiological investigation requested for conducting genome analysis and variant screening by real-time polymerase chain reaction (PCR) tests for SARS-CoV-2 (Administrative notice #0205-4 from the Director of Tuberculosis and Infectious Disease Control Division, Health Serviced Bureau of MHLW on February 5, 2021; partially revised on February 10, 2022)” and “Regarding the handling of hospital admissions and discharges, close contacts, and disclosure of patients with confirmed infection by the B.1.1.529 lineage (Omicron variant) (Administrative notice from MHLW on February 2, 2021)” promulgated by Article 15, the Act on the Prevention of Infectious Diseases and Medical Care for Patients with Infectious Diseases (Act No. 114 of October 2, 1998).
Recently, the MHLW and the National Institute of Infectious Diseases (NIID) have been concerned about the severe or fatal pediatric cases of SARS-CoV-2 infection as the number of pediatric cases increased 1), so we conducted an epidemiological investigation of fatal cases of SARS-CoV-2 infection in patients under 20 years old (fatal pediatric cases). Fatal pediatric cases included those caused both directly and indirectly by SARS-CoV-2 infection. We collaborated with three academic societies: the Japan Pediatric Society, the Japanese Society of Intensive Care Medicine, and the Japanese Association for Acute Medicine.
This record is an interim analysis of the fatal pediatric cases reported from January 1 to August 31, 2022.
Methods
Subjects who satisfied either of the following two conditions were included in the investigation. Research staff or fellows of the Field Epidemiology Training Program for NIID collected epidemiological data of local health authorities and visited medical institutions to collect data on medical records if possible and interview physicians (hereafter, field investigation).
Subjects investigated
1)Patients under 20 years old whose date of onset (or admission date) was on January 1, 2022, or later, and who died during the acute phase of infection with SARS-CoV-2.
2)Patients under 20 years old whose date of onset (or admission date) was on January 1, 2022, or later, and who died after the acute phase of infection with SARS-CoV-2 (including cases with other causes of death).
Items investigated
Age, sex, underlying disease, vaccine history of SARS-CoV-2 immunization, date of onset, date of death, symptoms/findings, disease suspected of causing death, and others.
Results (Interim)
A summary of the cases and results of the field investigation as of August 31, 2022, follows below. In collecting the information on the cases, it was difficult to classify the subjects into those exactly meeting criterion 1) or 2). Moreover, we have taken care to ensure that individuals are not identifiable.
〇 Summary of the cases
The total number of cases was 41 (age: <1 year old, n=8 [20%]; 1–4 years old, n=10 [24%]; 5–10 years old, n=17 [41%]; 12–19 years old, n=5 [12%]; and unknown, n=1 [2%]; sex: males, 23 cases [56%] and females, 18 cases [44%]). The figure shows the distribution of cases based on the date of onset after January 1, 2022 (epidemiological week 52, 2021). Cases have been continuously reported since January 2022 and started to increase from epidemiological week 28 (July 11–July 17).
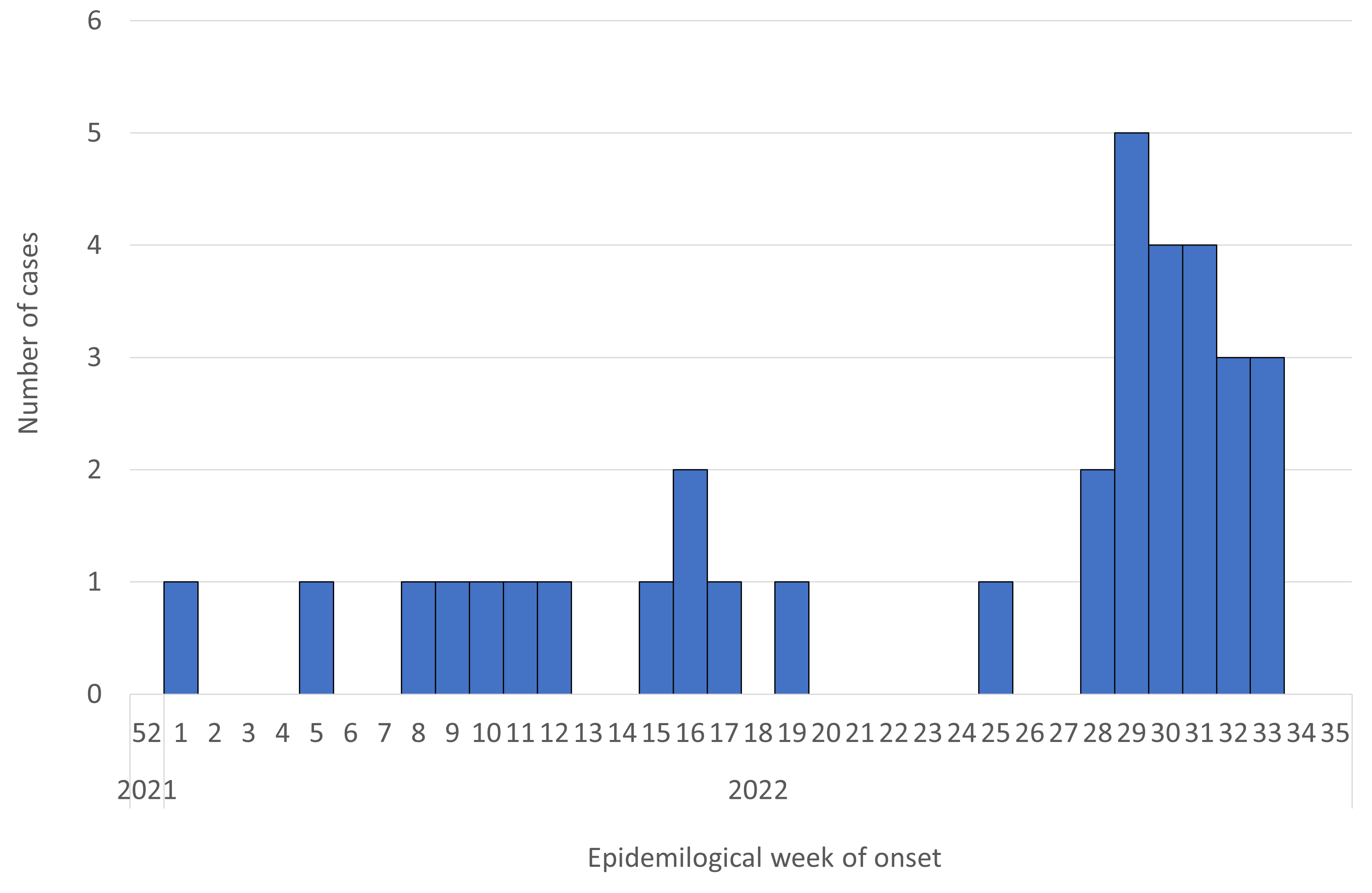
Figure. Reported number of deaths in patients under 20 years of age after SARS-CoV-2 infection (n=34*; date of onset or admission date from January 1, 2022 [week 52, 2021] to August 31, 2022 [week 35, 2022]) (as of August 31, 2022**)
* Seven cases were excluded for unknown date of onset.
** Case numbers in late August may not reflect the actual number of cases due to delayed reporting, so care must be taken in interpreting the data.
〇 Results of the field investigation
Of the 41 cases, we could conduct a field investigation of 32 cases. Among them, 29 cases were considered to be endogenous deaths (death due to other than trauma). The details of these 29 cases are as follows (Table).
Among the 29 cases, eight (28%) patients were <1 year old, six (21%) were 1–4 years old, 12 were 5–11 years old, and three (10%) were 12–19 years old, of whom 16 cases (55%) were in males and 13 cases (45%) were in females. Underlying disease was present in 14 (48%) patients and absent in 15 (52%). As of August 31, 2022, details of underlying disease, including duplicates, showed seven with central nervous system (CNS) abnormalities (50%), two with congenital heart disease (14%), and two with chromosomal abnormalities (14%). Among these 29 patients, 14 (48%) were not eligible for SARS-CoV-2 immunization and 15 (52%) were. Among the 15 patients eligible for SARS-CoV-2 immunization who were 5 years old or older, 13 (87%) were not vaccinated, and two (13%) were vaccinated twice, both of whom were 12 years old or older and whose last vaccination had been more than three months earlier. Moreover, a high number of symptoms or clinical findings on hospital arrival included fever in 23 cases (79%), nausea and/or vomiting in 15 (52%), disturbance of consciousness in 13 (45%), cough in nine (31%), inadequate intake of nutrition in nine (31%), seizure in eight (28%), and dyspnea in seven (24%). The main diseases suspected of causing death in medical institutions included cardiac abnormalities (n=7, 24%: myocarditis, arrhythmia, etc.), CNS abnormalities (n=7, 24%: acute encephalopathy, etc.), respiratory abnormalities (n=3, 10%: pneumonia, bacterial pneumonia, etc.), other diseases (n=6, 21%: multiple organ failure, etc.), and unknown cause of death (n=6, 21%). Several patients with a more rapid disease progression died due to CNS abnormalities such as encephalopathy, etc., and cardiac abnormalities such as myocarditis or arrhythmia. The date of onset was determined in 26 of the 29 cases, and the number of days from onset to death was a median of four days (range: 0–74 days), with eight patients (31%) dying in 0–2 days, 11 dying (42%) in 3–6 days, and seven dying (27%) in 7 days or more.
Of the 29 cases, 14 were thought to have underlying disease, including eight cases (57%) in patients under 5 years old (including four under one year old) and six cases (43%) in patients 6 years old or older. Nine cases (64%) were in males and five cases (36%) were in females. Symptoms or clinical findings on hospital arrival included fever in 11 cases (79%), dyspnea in seven (50%), nausea and/or vomiting in six (43%), cough in five (36%), inadequate intake of nutrition in four (29%), seizure in three (21%), and disturbance of consciousness in three cases (21%). In the medical institutions, the main diseases suspected of causing death were cardiac abnormality (n=3, 21%), respiratory abnormality (n=3, 21%), CNS abnormality (n=2, 14%), other disease (n=3, 21%), and unknown disease (n=3, 21%). Among these 14 cases, date of onset could be obtained in 12, and the number of days from onset to death was a median of four days (range: 1–74 days), with three patients (25%) dying in 0–3 days, seven dying (58%) in 3–6 days, and two dying (17%) in 7 days or more.
Of the 29 cases, 15 were considered to have no underlying disease. These included six cases (40%) in patients under five years old (including four under one year old) and nine cases (60%) in patients over 5 years old. Seven cases (47%) were in males and eight cases (53%) were in females. Symptoms or clinical findings on hospital arrival included fever in 12 cases (80%), disturbance of consciousness in 10 (67%), nausea and/or vomiting in nine (60%), seizure in five (33%), inadequate intake of nutrition in five (33%), cough in four (27%), and no cases (0%) with dyspnea. In the medical institutions, the main diseases suspected of causing death were CNS abnormalities (n=5, 33%), cardiac abnormalities (n=4, 27%), other disease (n=3, 20%), unknown cause of death (n=3, 20%), and respiratory abnormalities (n=0, 0%). Date of onset was obtained in 14 of the 15 cases, and the number of days from onset to death was a median of 4.5 days (range: 0–15 days), with five patients (36%) dying in 0–2 days, four dying (29%) in 3–6 days, and five dying (36%) in 7 days or more.
Table. Characteristics of fatal cases under 20 years of age after SARS-CoV-2 infection (n=29; limited to clearly endogenous deaths occurring only from January 1 to August 31, 2022; as of August 31, 2022)
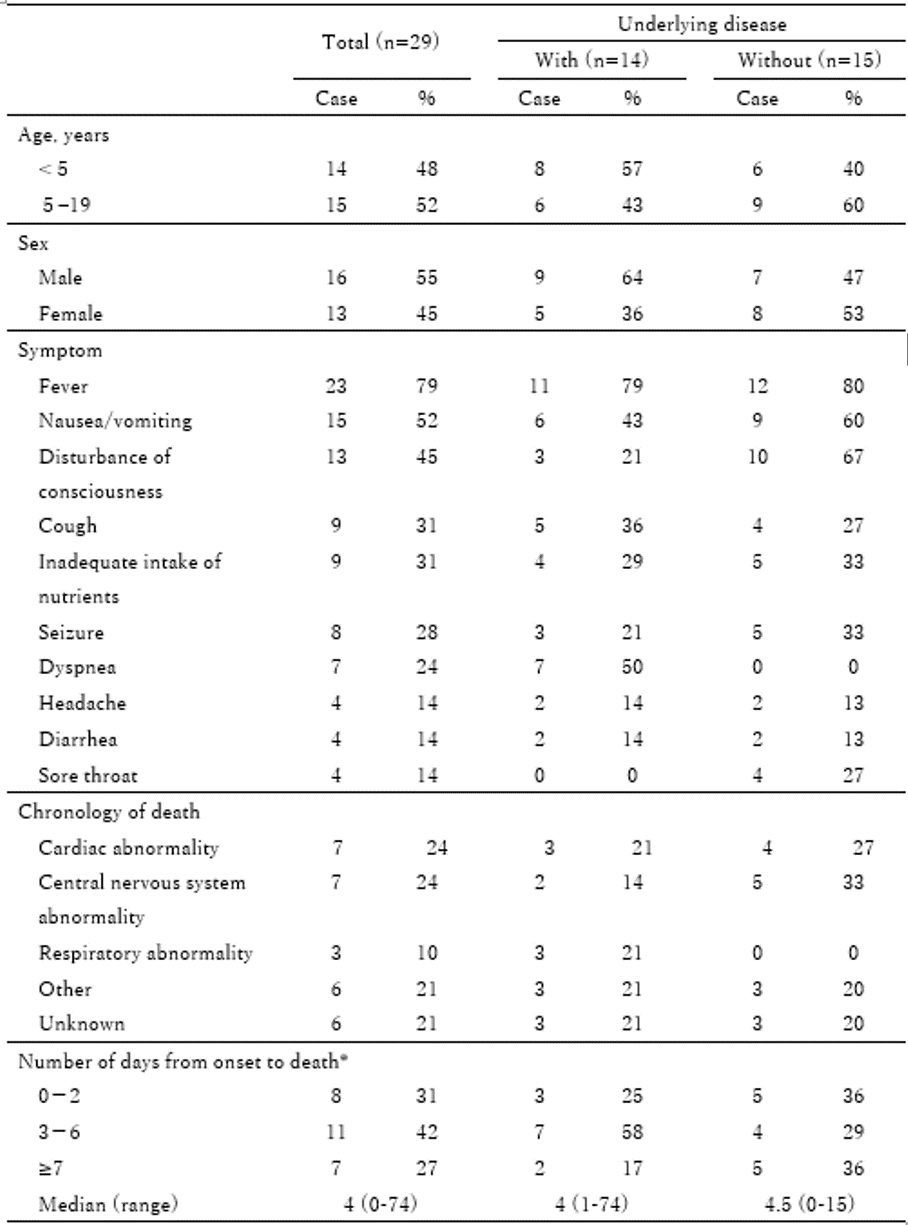
* Three cases whose date of onset or death was uncertain were excluded. Included were 12 cases with underlying disease and 14 cases without underlying disease.
Discussion
As of August 31, 2022, we described the interim report on 41 fatal pediatric cases from January 1 to August 31, 2022.
The number of cases had increased from mid-July 2022. In this field investigation, fatal pediatric cases caused by clearly endogenous factors included those in patients not only with underlying disease but also in patients with no underlying disease. Thus, families and healthcare workers might need to carefully follow the course of symptoms in those after SARS-CoV-2 infection. SARS-CoV-2 immunization was not administered in many of the fatal pediatric cases even though the children were of an approved age for the immunization. Moreover, compared to the registry of Japanese children with COVID-19 done by the Japan Pediatrics Society 2), the symptoms of the fatal pediatric cases in this investigation, except for respiratory symptoms, included a high proportion of nausea and/or vomiting (52%), disturbance of consciousness (45%), inadequate intake of nutrition (31%), and seizure (28%). The severity of COVID-19 is mainly classified only according to respiratory symptoms 3), but our results suggested that pediatric cases should be carefully followed up not only for respiratory symptoms but also for symptoms of CNS abnormalities such as disturbance of consciousness and seizure, vomiting, and inadequate intake of nutrients. The duration from onset to death was under one week in 73% of the patients, and our results further suggested that careful follow-up of the cases was important especially for the first week after onset of the disease.
Limitations and further investigation
This was an interim report as of August 31, 2022, and as the field investigation will continue to collect additional information on the fatal pediatric cases, the report may be revised and/or further information may be added, and we did not examine the causal relationship between SARS-CoV-2 infection and death. Therefore, the results should be carefully interpreted.We plan to continue to investigate fatal pediatric cases in cooperation with the local public health authorities and related academic associations.
Collaborating academic associations
Japan Pediatric Society, The Japanese Society of Intensive Care Medicine, Japanese Association for Acute Medicine.
References
1. Ministry of Health, Labour, and Welfare. Visualizing the data: information on COVID-19 infections. https://covid19.mhlw.go.jp/en/ (accessed on August 19, 2022).
2. Committee on Immunization and Prevention of Infectious Diseases, Japan Pediatric Society. Interim Report on Clinical Course of Domestic-Onset Pediatric Coronavirus Disease 2019 (COVID-19) Cases Using a Database: 3rd Report. Changes in Clinical Symptoms and Severity of Pediatric COVID-19 Cases Associated with the Omicron Epidemic. http://www.jpeds.or.jp/uploads/files/20220328_tyukan_hokoku3.pdf (accessed on August 19, 2022) [in Japanese].
3. Medical Treatment Guidance Review Committee. COVID-19 Treatment guidelines, the 8th Edition. https://www.mhlw.go.jp/content/000967699.pdf (accessed on August 19, 2022) [in Japanese].
- Details
掲載日:2022年9月14日
一部追加:2022年9月15日
国立感染症研究所実地疫学研究センター
同 感染症疫学センター
新型コロナウイルス感染症に罹患し、お亡くなりになった方々とご遺族の皆様に対し、深くお悔やみを申し上げます。
背景・目的
厚生労働省は、新型コロナウイルス(以下、「SARS-CoV-2」という。)感染による重症度等の知見を集積・監視するため、感染症の予防及び感染症の患者に対する医療に関する法律(平成10年法律第114号。)第15条に基づく積極的疫学調査の一環として、「新型コロナウイルス感染症の積極的疫学調査におけるゲノム解析及び変異株PCR検査について(要請)」(令和3年2月5日付け健感発0205第4号厚生労働省健康局結核感染症課長通知。令和4年2月10日一部改正。)及び「B.1.1.529系統(オミクロン株)の感染が確認された患者等に係る入退院及び濃厚接触者並びに公表等の取扱いについて」(令和3年11月30日付け厚生労働省新型コロナウイルス感染症対策推進本部事務連絡。令和4年2月2日一部改正。)において、自治体に対し、重症例及び死亡例についての報告やゲノム解析をこれまで依頼してきた。
今般、感染拡大に伴い、小児の感染者数が増加し1)、小児の重症例、死亡例発生への懸念から、厚生労働省及び国立感染症研究所は、関係学会(日本小児科学会、日本集中治療医学会、日本救急医学会)と協力して、SARS-CoV-2感染後の20歳未満の死亡例(以下、小児等の死亡例という。)について、急性期以降の死亡例も含め幅広く調査対象とし、積極的疫学調査を実施することとした。
本報告は、2022年1月1日から2022年8月31日までに報告された小児等の死亡例に関する暫定的な報告である。
方法
報告された小児等の死亡例のうち、下記2つのうちいずれかを満たす者を調査対象とした。自治体及び医療機関の協力のもと、国立感染症研究所職員及び実地疫学専門家養成コース研修員が、自治体による疫学調査等の資料収集、可能な限り現地に赴き実地においての医療機関での診療録の閲覧、及び医師への聞き取り等の調査(以下、実地調査という。)を実施した。
調査対象とした者:
①発症日(あるいは入院日)が2022年1月1日以降のSARS-CoV-2感染後の20歳未満の急性期の死亡例
②発症日(あるいは入院日)が2022年1月1日以降のSARS-CoV-2感染後の20歳未満の急性期以後に死亡した症例(死因を別原因とした症例。発症からの日数は問わない。)
実地調査における主な調査項目:
年齢、性別、基礎疾患、新型コロナワクチン接種歴、発症日、死亡日、症状/所見、死亡に至る経緯等
結果(暫定)
本調査における2022年8月31日現在の症例の概要、及び実地調査の結果は、以下のとおりであった。症例の収集において、調査対象を上述の①または②を満たす者としたが、報告された症例について①と②を明確に分類することは困難であった。なお、下記の記述内容は個人が特定されないよう配慮した。
〇症例の概要
症例は、2022年8月31日時点で、計41例(年齢:0歳8例(20%)、1-4歳10例(24%)、5-11歳17例(41%)、12-19歳5例(12%)、不明1例(2%)、性別:男性23例(56%)、女性18例(44%)、基礎疾患:あり18例(44%)、なし17例(41%)、不明6例(15%))であった。2022年1月1日(疫学週2021年52週)以降の発症日に基づく報告数を図に示した。症例は、2022年1月から継続的に発生し、疫学週2022年28週(7月11日~7月17日)から増加した。
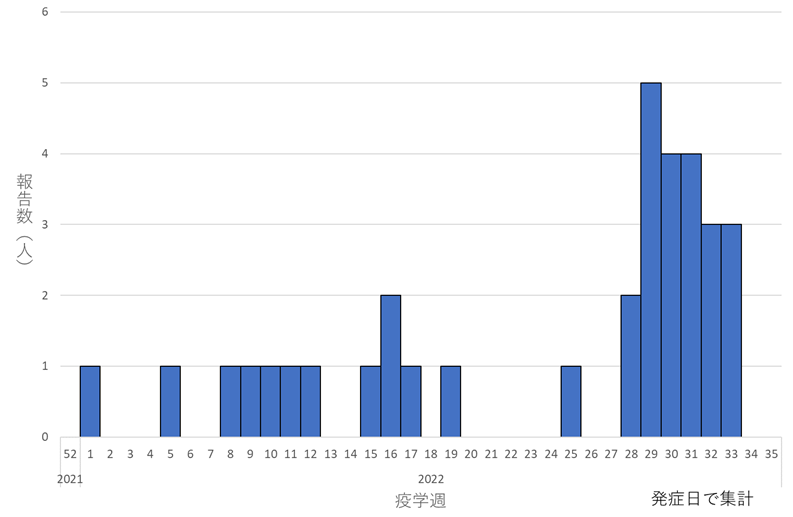
図.新型コロナウイルス感染後の20歳未満の死亡例の報告数(n=34*; 発症日または入院日が2022年1月1日(疫学週2021年52週)~8月31日(疫学週2022年35週))(2022年8月31日時点)**
*発症日不明の7例を除く
**直近の報告はグラフに反映されにくいため、解釈には注意が必要である。
〇実地調査の結果
41例のうち実地調査が実施できた症例は、2022年8月31日時点で32例であり、このうち、明らかな内因性死亡(外傷を除く疾病による死亡)と考えられたのは29例であった。以下、この29例について述べる(表)。
年齢・年代の内訳は、0歳8例(28%)、1-4歳6例(21%)、5-11歳12例(41%)、12-19歳3例(10%)であった。性別は、男性16例(55%)、女性13例(45%)であった。基礎疾患は、あり14例(48%)、なし15例(52%)であった。2022年8月31日時点での基礎疾患ありの内訳は、中枢神経疾患7例(50%)、先天性心疾患2例(14%)、染色体異常2例(14%)等であった(重複あり)。新型コロナワクチンは、29例のうち接種対象外年齢の者が14例(48%)、接種対象年齢の者が15例(52%)であり、接種対象年齢となる5歳以上の15例では、未接種が13例(87%)、2回接種が2例(13%)であった。接種を受けた2例はともに12歳以上であり、発症日は、最終接種日から最低3ヶ月を経過していた。また、医療機関到着時の症状/所見は、発熱23例(79%)、悪心嘔吐15例(52%)、意識障害13例(45%)、咳嗽9例(31%)、経口摂取不良9例(31%)、痙攣8例(28%)、呼吸困難7例(24%)の順に多かった。医療機関において疑われた死亡に至る主な経緯は、循環器系の異常7例(24%:心筋炎、不整脈等)、中枢神経系の異常7例(24%:急性脳症等)、呼吸器系の異常3例(10%:肺炎、細菌性肺炎等)、その他6例(21%:多臓器不全等)、原因不明6例(21%)であった。急性脳症等の中枢神経系の異常、心筋炎や不整脈等の循環器系の異常によって急激な経過を辿った症例があった。発症日は、29例のうち26例について得られ、発症から死亡までの日数が、中央値4日(範囲:0-74日)、内訳は0-2日が8例(31%)、3-6日が11例(42%)、7日以上が7例(27%)であった。
29例のうち基礎疾患があったと考えられた14例について、年齢・年代の内訳は、5歳未満8例(57%)(うち0歳4例)、5歳以上6例(43%)であった。性別は、男性9例(64%)、女性5例(36%)であった。医療機関到着時の症状/所見は、発熱11例(79%)、呼吸困難7例(50%)、悪心嘔吐6例(43%)、咳嗽5例(36%)、経口摂取不良4例(29%)、痙攣3例(21%)、意識障害3例(21%)であった。医療機関において疑われた死亡に至る主な経緯として、循環器系の異常3例(21%)、呼吸器系の異常3例(21%)、中枢神経系の異常2例(14%)、その他3例(21%)、原因不明3例(21%)であった。発症日は、14例のうち12例について得られ、発症から死亡までの日数は、中央値4日(範囲:1-74日)、内訳は0-2日が3例(25%)、3-6日が7例(58%)、7日以上が2例(17%)であった。
29例のうち基礎疾患がなかったと考えられた15例について、年齢・年代の内訳は、5歳未満6例(40%)(うち0歳4例)、5歳以上9例(60%)であった。性別は、男性7例(47%)、女性8例(53%)であった。医療機関到着時の症状/所見は、発熱12例(80%)、意識障害10例(67%)、悪心嘔吐9例(60%)、痙攣5例(33%)、経口摂取不良5例(33%)、咳嗽4例(27%)、呼吸困難0例(0%)であった。医療機関において疑われた死亡に至る主な経緯は、中枢神経系の異常5例(33%)、循環器系の異常4例(27%)、その他3例(20%)、原因不明3例(20%)であり、呼吸器系の異常はなかった。発症日は、15例のうち14例について得られ、発症から死亡までの日数は、中央値4.5日(範囲:0-15日)、内訳は0-2日が5例(36%)、3-6日が4例(29%)、7日以上が5例(36%)であった。
表. 新型コロナウイルス感染後の20歳未満の死亡例の特性
(n=29 ; 発症日または入院日が2022年1月1日から8月31日、明らかな内因性死亡に限る)(2022年8月31日時点)
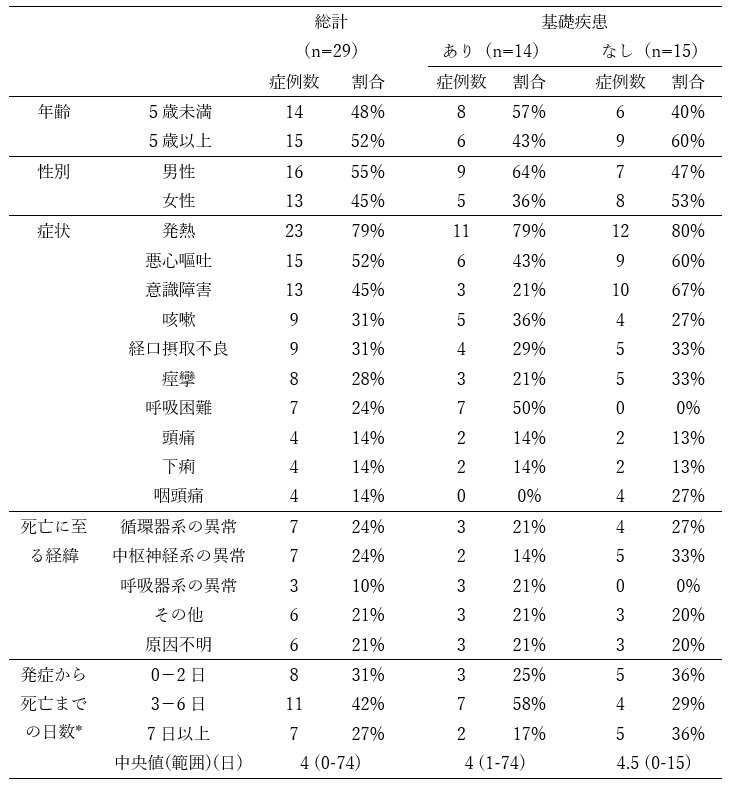
* 発症から死亡までの日数は発症日に関する情報が得られた26例(基礎疾患あり12例、基礎疾患なし14例)
考察
2022年8月31日時点における、2022年1月1日から2022年8月31日までに報告された小児等の死亡例、41例について暫定的な報告を行った。症例数は、7月中旬から増加していた。
今回の実地調査で内因性死亡が明らかとされた小児等の死亡例において、基礎疾患のなかった症例も死亡していることから、SARS-CoV-2感染後は、基礎疾患のある者はもちろん、基礎疾患のない者においても、症状の経過を注意深く観察することが必要であると考えられた。新型コロナワクチンは、接種対象でも多くの小児の死亡例では未接種であった。また、症状は、日本小児科学会による国内小児におけるCOVID-19レジストリ調査2)と比較して、呼吸器症状以外の症状のうち、悪心嘔吐(52%)、意識障害(45%)、経口摂取不良(31%)、痙攣(28%)の割合が高かった。新型コロナウイルス感染症における重症度分類は、主に呼吸器症状等により分類されているが3)、小児においては、痙攣、意識障害などの神経症状や、嘔吐、経口摂取不良等の呼吸器症状以外の全身症状の出現にも注意を払う必要があると考えられた。発症から死亡までの日数は、1週間未満が73%を占めており、特に発症後1週間の症状の経過観察が重要であると考えられた。
調査に関する制限と今後
本報告は、2022年8月31日時点での暫定的な報告であり、今後の調査の進捗にあわせて、情報の更新・修正がなされる可能性がある点、及び本調査では、SARS-CoV-2感染と死亡との因果関係を検討していない点に留意する必要がある。引き続き、自治体及び関係学会の協力のもと、本調査を継続していく予定である。
本調査における協力学会:日本小児科学会、日本集中治療医学会、日本救急医学会
謝辞:本調査にご協力いただきました関係者の皆様に心より御礼申し上げます。
参考資料:
1. 厚生労働省 データからわかる-新型コロナウイルス感染症情報
https://covid19.mhlw.go.jp/ (閲覧日:2022年8月19日)
2. 小児科学会 予防接種・感染症対策委員会「データベースを用いた国内発症小児 Coronavirus Disease 2019 (COVID-19) 症例の臨床経過に関する検討」の中間報告:第3報、2022年3月28日
http://www.jpeds.or.jp/uploads/files/20220328_tyukan_hokoku3.pdf
3. 新型コロナウイルス感染症診療の手引き・第8.0版
https://www.mhlw.go.jp/content/000967699.pdf
追加:(2022/9/15)参考資料1.の引用表記を追記しました。