Infectious Deseases
Basic Research
Surveillance
Information
- Details
71th meeting of the COVID-19 advisory boardof Ministry of Health, Labour and Welfare (February 9, 2022). Material 1
Evaluation of the latest infection status, etc.
Infection status
- The number of new cases of infection (by date of report) nationwide increased continuously to approximately 505 per 100,000 in the latest week. However, at the same time, the ratio of new cases to that for the previous week is 1.19, indicating a continuous downward trend, with an increasing pace. Seen by age group, the proportion of patients in their 20s has decreased, while the proportions of patients under 10 years old and patients in their 60s and older has increased.
- Among the 35 prefectures that are currently under priority measures, Shimane, Hiroshima, Yamaguchi, Nagasaki, Kumamoto, Miyazaki, and Okinawa show a downward trend or a sign of bottoming out in the number of new cases of infection, with a ratio to that for the previous week of less than 1. Gunma is also showing signs of a decrease, with a ratio to that for the previous week of 0.99. In other prefectures, the ratio to that for the previous week is also on a downward trend, showing continuous slowing, with an increasing pace. In Okinawa, where the number of new cases of infection continues to decrease, all age groups are showing a decrease. Among prefectures where priority measures are not in force, Akita, Yamanashi, Tottori, and Ehime have a ratio to that for the previous week of less than 1.
- While the pace of increase in the number of new cases of infection is slowing down nationwide, the numbers of patients receiving treatment, severe patients, and deaths continue to increase.
- In the Tokyo metropolitan area and Kansai area, cases of infection with the Omicron variant have become dominant.
Effective reproduction number: On a national basis, the most recent number is above 1 (1.07; as of January 24), while the figure stands at 1.09 in the Tokyo metropolitan area and 1.06 in the Kansai area.
Local trends
* The value for new cases of infection is the number of persons per 100,000 among the total number for the latest week, based on reporting dates.
< Areas under priority measures >
- Hokkaido
The number of new cases of infection has increased continuously to approximately 459 (approximately 669 in Sapporo City), with a ratio to that for the previous week of 1.30. The infected individuals are mainly in their 30s or younger. The use rate of beds is approximately 30%.
- Tohoku
In Aomori, the number of new cases of infection has increased continuously to approximately 221, with a ratio to that for the previous week of 1.18. The infected individuals are mainly in their 30s or younger. The use rate of beds is slightly more than 30%. In Yamagata and Fukushima, the number of new cases of infection has also increased continuously, to approximately 171 and 194, respectively. Both prefectures show an increase, with a ratio to that for the previous week of more than 1. The use rate of beds is slightly more than 40% in Yamagata and Fukushima.
- North Kanto
In Gunma, the number of new cases of infection is approximately 347, with a ratio to that for the previous week of less than 1 (0.99). The infected individuals are mainly in their 30s or younger. The use rate of beds is slightly less than 60%. In Ibaraki and Tochigi, the number of new cases of infection has increased continuously, to approximately 346 and 300, respectively. Both prefectures show an increase, with a ratio to that for the previous week of more than 1. The use rate of beds is slightly more than 30% in Ibaraki and Tochigi.
- Tokyo metropolitan area(Tokyo and 3 neighboring prefectures)
Tokyo continues to show an increase in the number of new cases of infection. The number has reached the highest value in Japan (approximately 926), with a ratio to that for the previous week of 1.21. The infected individuals are mainly in their 30s or younger, while the number of those aged less than 10 years is also increasing. The use rate of beds is slightly more than 50%, while the use rate of beds for severe patients is approximately 40%. In Saitama, Chiba, and Kanagawa, the number of new cases of infection has also increased continuously, to approximately 550, 537, and 613, respectively. All of these prefectures show an increase, with a ratio to that for the previous week of more than 1. The use rate of beds is slightly less than 70% in Saitama, slightly more than 60% in Chiba, and slightly less than 70% in Kanagawa. The use rate of beds for severe patients is approximately 40% in Kanagawa.
- Chubu/Hokuriku
In Ishikawa, the number of new cases of infection has increased continuously to approximately 297, with a ratio to that for the previous week of 1.20. The infected individuals are mainly in their 30s or younger. The use rate of beds is slightly more than 50%. In Niigata and Nagano, the number of new cases of infection has also increased continuously, to approximately 156 and 193, respectively. The use rate of beds is slightly more than 30% in Niigata and slightly more than 90% in Nagano.
- Chukyo/Tokai
In Aichi, the number of new cases of infection has increased continuously to approximately 521, with a ratio to that for the previous week of 1.13. The infected individuals are mainly in their 30s or younger. The use rate of beds is slightly more than 50%. In Gifu, Shizuoka, and Mie, the number of new cases of infection has also increased continuously, to approximately 302, 324, and 292, respectively. All of these prefectures show an increase, with a ratio to that for the previous week of more than 1. The use rate of beds is slightly more than 50% in Gifu and Shizuoka, and slightly less than 50% in Mie.
- Kansai area
In Osaka, the number of new cases of infection has increased continuously to approximately 871, with a ratio to that for the previous week of 1.15. The infected individuals are mainly in their 30s or younger. The use rate of beds is approximately 90%, while the use rate of beds for severe patients is slightly more than 40%. In Kyoto, Hyogo, and Wakayama, the number of new cases of infection has also increased continuously, to approximately 689, 714, and 387, respectively. All of these prefectures show an increase, with a ratio to that for the previous week of more than 1. The use rate of beds is slightly less than 60% in Kyoto and slightly more than 70% in Hyogo. The use rate of beds for severe patients is slightly more than 50% in Kyoto and slightly more than 20% in Hyogo.
- Chugoku/Shikoku
In Hiroshima, the number of new cases of infection is approximately 267, with a ratio to that for the previous week of less than 1 (0.81). The infected individuals are mainly in their 30s or younger. The use rate of beds is slightly more than 50%, while the use rate of beds for severe patients is slightly more than 30%. In Shimane and Yamaguchi, the number of new cases of infection has also decreased to approximately 77 and 161, respectively, with a ratio to that for the previous week of less than 1 (0.89 and 0.85, respectively). In Okayama and Kagawa, the number of new cases of infection has increased continuously, to approximately 391 and 246, respectively. Both prefectures show a continuous increase, with a ratio to that for the previous week of more than 1. The use rate of beds is approximately 30% in Shimane, slightly more than 50% in Okayama, slightly more than 40% in Yamaguchi, and slightly more than 50% in Kagawa.
- Kyushu
In Fukuoka, the number of new cases of infection has increased continuously to approximately 642, with a ratio to that for the previous week of 1.17. The infected individuals are mainly in their 30s or younger. The use rate of beds is slightly more than 80%. In Saga, Oita, and Kagoshima, the number of new cases of infection has increased continuously, to approximately 432, 269, and 263, respectively. All of these prefectures show an increase, with a ratio to that for the previous week of more than 1. In Nagasaki, Kumamoto, and Miyazaki, the number of new cases of infection is 276, 344, and 213, respectively, with a ratio to that for the previous week of less than 1 (0.91, 0.85. and 0.86, respectively). The use rate of beds is slightly more than 30% in Saga, slightly more than 40% in Nagasaki and Miyazaki, slightly more than 60% in Kumamoto, slightly more than 40% in Oita, and slightly less than 60% in Kagoshima. The use rate of beds for severe patients is slightly more than 20% in Kumamoto.
- Okinawa
The number of new cases of infection is approximately 295, and the ratio to that for the previous week remains less than 1 (0.67). In the Yaeyama district, the increase is continuing. The newly infected individuals are mainly in their 30s or younger. The use rate of beds is approximately 60%, while the use rate of beds for severe patients is slightly more than 50%.
< Areas other that the above >
-
In Iwate, Miyagi, Toyama, Fukui, Shiga, Nara, Tokushima, and Kochi, the number of new cases of infection is approximately 84, 198, 203, 200, 496, 516, 169, and 225, respectively. All of these prefectures show an increase, with a ratio to that for the previous week of more than 1. In Akita, Yamanashi, Tottori, and Ehime, the number of new cases of infection is 132, 235, 122, and 133, respectively, with a ratio to that for the previous week of less than 1 (0.82, 0.82, 0.65, and 0.87, respectively). The use rate of beds is slightly more than 40% in Iwate, slightly more than 30% in Miyagi, Akita, Toyama, and Tokushima, approximately 20% in Fukui, slightly more than 50% in Yamanashi, approximately 60% in Shiga, slightly more than 70% in Nara, slightly more than 20% in Tottori, slightly less than 40% in Ehime, and approximately 40% in Kochi.
Future outlook and measures to be taken
- The nationwide number of new cases of infection continues to increase, while its pace is slowing down. The infection still seems to occur at certain places, such as homes, schools, nursery schools, workplaces, and nursing welfare facilities. The nighttime population is generally decreasing in the areas under priority measures, although it is increasing in some areas. In some areas, the number of new cases of infection has been decreasing or stopped increasing. As its ratio to that for the previous week and the effective reproduction number by date of report are approaching 1 even in large cities, the number of new cases of infection may peak in the future. However, attention should be paid to the fact that possible discrepancies have been pointed out between the published data and the actual status, due to delayed reporting and a strained testing system, as well as the possibility that the number may increase again when the Omicron variant (BA.2) becomes dominant in the future.
- Individuals infected with the Delta variant, which is more likely to cause severe symptoms, are still being detected, although their number is decreasing, along with replacement by the Omicron variant. In Okinawa, where a prevalence of infection with the Omicron variant was seen earlier than in other areas, the number of new cases of infection has been decreasing, while there was a lag of approximately 2 weeks in the timing when the number of patients staying at hospitals or other facilities began to decrease. In addition, a similar trend was seen in the course of the infection, until the number of infected individuals at nursing welfare facilities began to decrease.
- Even if the number of new cases of infection decreases mainly among young people in many areas, medical care provision system and other types of service for mild and moderate patients will continue to remain strained for a while, and the possibility that there will be limited bed availability for severe patients will become higher, along with a possible increase in the number of elderly patients with severe symptoms. Attention should also be given to a possible increase in the number of infected individuals requiring hospitalization, as test-positive persons with an underlying disease may require hospitalization due to disease exacerbation by the infection, even in cases where they do not have COVID-19 pneumonia.
- Each year, many cases of emergency transportation usually occur during this period. According to a status survey on cases of emergency transportation difficulties, cases of suspected non-COVID-19 have increased compared to cases of suspected COVID-19, in many municipalities. With a rapid increase in the number of cases of suspected COVID-19, cases of emergency transportation difficulties have exceeded those during the same period last year and during the spread of the infection last summer. There is already a significant burden on regular medical care, especially emergency medical care.
Findings on the characteristics of the Omicron variant
- [Infectivity/transmissibility]
It has been confirmed that compared to the Delta variant, the generation time has shortened to approximately 2 days (approximately 5 days for Delta). The doubling time and incubation period have also shortened, the risk of re-infection and secondary infection after infection has increased, and the speed of infection spread is very fast. As the obtained data indicates that the serial interval is shorter than the incubation period in individuals infected with the Omicron variant, its transmission before disease onset probably occurs to a certain extent, as in the case of infection with the conventional strain.
- [Place/route of infection]
In Japan, many cases of infection occur through the same opportunities as before (spending time indoors with insufficient ventilation, eating and drinking, etc.), and infection is considered to occur via the same routes as before (droplets, aerosol inhalation, contact infection, etc.).
- [Severity]
It has been suggested that infection with the Omicron variant may present a relatively lower risk of hospitalization and aggravation than does the Delta variant. However, the number of cases of hospitalization due to the Omicron variant infection has already increased.
- [Duration of viral shedding]
Viral shedding in individuals infected with the Omicron variant decreases over time, regardless of vaccination status. In patients with symptoms, it has been shown that the possibility of viral shedding after Day 10 (when the date of onset is regarded as Day 0) is as low as in the case of infection with the conventional strain. In patients with no symptoms, it has been shown that the possibility of viral shedding is low 8 days after the date of diagnosis.
- [Vaccine effect]
For infection with the Omicron variant, the preventive effect of a first vaccination against disease onset is markedly reduced, but its preventive effect on hospitalization is maintained at a certain level. It has also been reported that a booster shot improves the preventive effects against disease onset and hospitalization for infection with the Omicron variant.
- [BA.2 lineage]
In some areas overseas, the number of cases of infection with the BA.2 lineage is increasing. Currently, the mainstream of the Omicron variant in Japan is the BA.1 lineage, but the BA.2 lineage has also been detected in quarantine and in Japan. Monitoring must be continued through a certain number of genome analyses. Analyses of the effective reproduction number, risk of domestic secondary infection, and other indices have shown that the infectivity of the BA.2 lineage is higher than that of the BA.1 lineage. According to a report from Denmark, there is no difference in the risk of hospitalization between the BA.1 lineage and the BA.2 lineage, in terms of severity. In addition, a report from the UK says that there is no difference in the preventive effect of vaccination between these lineages.
Efforts based on the spread of infection due to the Omicron variant
- [Test/diagnosis and surveillance in areas with a rapid spread of infection]
A test/diagnosis system and the processing of notifications to public health centers are becoming strained, and there are concerns regarding discrepancies between the published data and the actual status. It is necessary to consider effective and appropriate surveillance, in order to properly grasp the trend of occurrences. Tests and active epidemiological surveys should be prioritized based on the findings obtained thus far. Regarding free tests for people who are worried about infection and wish to undergo testing, attention should be paid to a rapid increase in demand for tests as well as test availability, and a system to ensure prioritized testing needs to be secured.
- [Monitoring system for mutant strains in Japan]
While the infection is spreading nationwide, it is necessary to maintain a surveillance system according to the local infection status, including the situation regarding replacement with the Omicron variant. For severe patients, clusters, or other applicable cases, a genome analysis should also be performed to identify variants such as the Delta variant.
- [Measures taken by local governments]
Based on the infection status of the region and forecasts of the numbers of infected cases and severe cases, local governments must work flexibly to secure the required number of beds and healthcare professionals, secure the functions of public health centers, which are indispensable for local communities, along with support for strengthening the healthcare center system, and establish home-visit and online medical care systems for home care recipients. At that time, it is necessary to secure a system for prompt administration of oral therapeutic drugs and neutralizing antibody drugs, for patients at risk of developing severe disease, such as elderly patients and patients with underlying diseases. As patients with acute diseases other than COVID-19 who require emergency transportation often appear during the winter, attention should be given to the balance between medical care for COVID-19 and regular medical care. If the infection spreads rapidly, it will be necessary to secure prompt access to consultation and condition monitoring for those at a higher risk of developing severe disease. Furthermore, it is also necessary to establish a system that enables COVID-19 patients with an underlying disease to continue treatment for the underlying disease.
- [Reinforcement of information provision to persons who have not been vaccinated or who are eligible for booster vaccination]
Local governments are required to promote the provision of information on vaccination. Booster vaccinations, which have already been started, must also be implemented steadily, along with vaccinations for unvaccinated persons. The number of infected individuals among the elderly may continue to increase in the future. Therefore, it is necessary to further accelerate vaccinations for the elderly and other eligible persons, and also to successively provide vaccination services ahead of the original schedule for the general public as well, as much as possible.
- [Quarantine measures]
The waiting period after entering Japan has been further reduced from 10 days to 7 days. It is necessary to continue to verify future quarantine measures, while taking into account the prevalence of variants such as the Omicron variant in Japan and overseas. For individuals found to be positive by an entrance test, a whole-genome analysis should continue to be performed, to monitor the strains that are spreading overseas.
Strengthening and thorough implementation of infection prevention measures based on the characteristics of the Omicron variant
-
Based on the situation where the infection is spreading due to the Omicron variant, a proposal has just been made at the meeting of the Subcommittee on Novel Coronavirus Disease Control held on February 4. In situations/places where the infection is spreading, prevention measures based on the characteristics of the Omicron variant should be strengthened and thoroughly implemented.
- In many areas, the numbers of persons who are positive for the COVID-19 and in close contact with infected individuals are increasing at schools, kindergartens, nursery schools, etc. Local governments need to actively promote vaccination for teachers, childcare workers, and the other staff at such facilities. It is also necessary to consider securing educational opportunities through multiple measures including staggered attendance and online lessons, and maintaining social functions.
- At nursing welfare facilities, promotion of booster vaccinations for residents and staff, as well as aggressive testing for staff is required. For infection control and medical care at facilities, external support is important.
- At workplaces, it is necessary to promptly review business continuity plans, and to reduce staff attendance at workplaces and opportunities for contact by utilizing telework, promoting the taking of time off, and through other measures, so that social functions can be maintained. Thorough health management and active promotion of occupational booster vaccinations for workers are also needed.
It is essential to widely share the current infection status with citizens and business operators, and cooperate toward preventing the spread of infection.
- Basic preventative measures are still effective against infection with the Omicron variant. Therefore, administrative officers, business operators, and citizens should continue to ensure the proper wearing of nonwoven masks, hand washing, ventilation, etc. The risk of infection becomes highest when the three Cs (crowded places, closed spaces, and close contact) overlap. However, even a single C should be avoided, as much as possible, because the Omicron variant is highly transmissible. Booster vaccinations are also effective in preventing disease aggravation/onset.
- When going out, it is necessary to avoid situations/places with a high risk of infection such as crowds, and large gatherings either with or without shouting/loud speaking in poorly ventilated spaces. Activities with other persons should be carried out in a small group of people who usually meet each other. Eating and drinking together should be carried out in a small group, without speaking to the extent possible, in principle, and the wearing of masks should be ensured at all times, except while eating and drinking.
- In order to protect the lives of both ourselves and our families, and at the same time, to prevent the spread of infection due to the Omicron variant, it is necessary to refrain from going out if you feel a little unwell, such as a mild fever or fatigue, and to consult a physician and undergo tests according to government policy.
Figures (Number of new infections reported etc.) (PDF)
- Details
70th meeting of the COVID-19 advisory board of Ministry of Health, Labour and Welfare (February 2, 2022). Material 1
Evaluation of the latest infection status, etc.
Infection status
- The number of new cases of infection (by date of report) nationwide increased continuously to approximately 426 per 100,000 in the latest week. However, at the same time, its ratio to that for the previous week is 1.5, indicating a continuous downward trend, with an increasing pace. The number of new cases of infection has increased mainly, in people in their 20s or younger. Seen by age group, the proportion of patients in their 20s has decreased, while the proportion of patients under 10 years old has increased.
- Among the 34 prefectures that are currently under priority preventative measures, 31 prefectures (other than Okinawa, Shimane, and Hiroshima) are continuing to show an increase. Nearly all prefectures that are under priority measures have a ratio of new cases for this week to that for the previous week of 2 or lower; however, some areas continue to show a rapid increase, with a ratio of more than 2. On the other hand, Okinawa continues to show a decrease, with a ratio of new cases for this week to that for the previous week of less than 1. However, it should be noted that although the number of new cases of infection is decreasing in young people, mainly in those in their 20s, it is increasing in elderly people in their 70s.
- In 13 prefectures where priority measures are not in force, some areas continue to show a rapid increase in the number of new cases of infection, with a ratio to that for the previous week of more than 2.
- With the continued increase in the number of new cases of infection nationwide, both a rapid increase in the number of patients receiving treatment and an increase in the number of severe patients continue to be seen.
- Although the Delta variant is still being detected, it has nearly been replaced by the Omicron variant in the Tokyo metropolitan area and the Kansai area.
Effective reproduction number: On a national basis, the most recent number is above 1 (1.19; as of January 17), and the figure stands at 1.23 in the Tokyo metropolitan area and 1.19 in the Kansai area.
Local trends
* The value for new cases of infection is the number of persons per 100,000 among the total number for the latest week, based on reporting dates.
< Area subject to priority measures >
- Hokkaido
The number of new cases of infection has increased continuously to approximately 353 (approximately 505 in Sapporo City), with a ratio to that for the previous week of 1.7. The infected individuals are mainly in their 30s or younger. The use rate of beds is slightly less than 30%.
- Tohoku
In Aomori, the number of new cases of infection has increased continuously to approximately 186, with a ratio to that for the previous week of 1.7. The infected individuals are mainly in their 20s or younger. The use rate of beds is slightly more than 20%. In Yamagata and Fukushima, the number of new cases of infection has also increased continuously, to approximately 132 and 152, respectively. Both prefectures show a rapid increase, with a ratio to that for the previous week of more than 2. The use rate of beds is slightly more than 20% in Yamagata and slightly more than 40% in Fukushima.
- North Kanto
In Gunma, the number of new cases of infection has increased continuously to approximately 349, with a ratio to that for the previous week of 1.5. The infected individuals are mainly in their 30s or younger. The use rate of beds is slightly more than 50%. In Ibaraki and Tochigi, the number of new cases of infection has also increased continuously, to approximately 222 and 230, respectively. Both prefectures show an increase, with a ratio to that for the previous week of more than 1. The use rate of beds is slightly more than 30% in both prefectures.
- Metropolitan area (Tokyo and 3 neignboring prefectures)
Tokyo continues to show a rapid increase in the number of new cases of infection. The number has reached the highest value in Japan (approximately 767), with a ratio to that for the previous week of 1.6. The infected individuals are mainly in their 20s and 30s, while the number of those aged less than 10 years are also increasing. The use rate of beds is slightly less than 50%, while the use rate of beds for severe patients is slightly more than 30%. In Saitama, Chiba, and Kanagawa, the number of new cases of infection has also increased continuously, to approximately 399, 392, and 504, respectively. Both prefectures show an increase, with a ratio to that for the previous week of more than 1. The use rate of beds is slightly less than 60% in Saitama, and slightly less than 50% in Chiba and Kanagawa.
- Chubu/Hokuriku
In Ishikawa, the number of new cases of infection has increased continuously to approximately 248, with a ratio to that for the previous week of 1.7. The infected individuals are mainly in their 20s or younger. The use rate of beds is slightly more than 40%. In Niigata and Nagano, the number of new cases of infection has also increased continuously, to approximately 152 and 189, respectively. Both prefectures show an increase, with a ratio to that for the previous week of more than 1. The use rate of beds is slightly more than 20% in Niigata and slightly more than 60% in Nagano.
- Chukyo/Tokai
In Aichi, the number of new cases of infection has increased continuously to approximately 462, with a ratio to that for the previous week of 1.6. The infected individuals are mainly in their 30s or younger. The use rate of beds is slightly more than 50%. In Gifu, Shizuoka, and Mie, the number of new cases of infection has also increased continuously, to approximately 273, 276, and 231, respectively. Both prefectures show an increase, with a ratio to that for the previous week of more than 1. The use rate of beds is slightly more than 60% in Gifu, slightly more than 30% in Shizuoka, and slightly more than 40% in Mie.
- Kansai area
In Osaka, the number of new cases of infection has increased continuously to approximately 760, with a ratio to that for the previous week of 1.5. The infected individuals are mainly in their 30s or younger. The use rate of beds is slightly more than 70%, while the use rate of beds for severe patients is slightly more than 30%. In Kyoto and Hyogo, the number of new cases of infection has also increased continuously, to approximately 600 and 549, respectively. Both prefectures show an increase, with a ratio to that for the previous week of more than 1. The use rate of beds is slightly more than 50% in Kyoto and slightly more than 60% in Hyogo. The use rate of beds for severe patients is approximately 40% in Kyoto.
- Chugoku/Shikoku
In Hiroshima, the number of new cases of infection is approximately 328, with a ratio to that for the previous week of less than 1 (0.98). The infected individuals are mainly in their 30s or younger. The use rate of beds is approximately 50%, while the use rate of beds for severe patients is slightly more than 20%. In Okayama, Yamaguchi, and Kagawa, the number of new cases of infection has also increased continuously, to approximately 320, 190, and 241, respectively. In Shimane, the number of new cases of infection has decreased to approximately 87, with a ratio to that for the previous week of less than 1 (0.5). In Okayama, Yamaguchi, and Kagawa, the number of new cases is continuing to increase, with a ratio to that for the previous week of more than 1. The use rate of beds is slightly more than 30% in Shimane, slightly more than 40% in Okayama, approximately 50% in Yamaguchi, and slightly more than 30% in Kagawa.
- Kyushu
In Fukuoka, the number of new cases of infection has increased continuously to approximately 548, with a ratio to that for the previous week of 1.6. The infected individuals are mainly in their 30s or younger. The use rate of beds is slightly less than 50%. In Saga, Nagasaki, Kumamoto, Oita, Miyazaki, and Kagoshima, the number of new cases of infection has increased continuously, to approximately 362, 302, 406, 247, 247, and 248, respectively. Both prefectures show an increase, with a ratio to that for the previous week of more than 1. The use rate of beds is approximately 40% in Saga, slightly less than 40% in Nagasaki and Miyazaki, slightly more than 70% in Kumamoto, slightly more than 40% in Oita, and slightly more than 50% in Kagoshima.
- Okinawa
The number of new cases of infection is approximately 439, and the ratio to that for the previous week remains less than 1 (0.8). In the Yaeyama district, the increase is continuing. The newly infected individuals are mainly in their 30s or younger, while the number of those in their 70s is increasing. The use rate of beds is slightly less than 70%, while the use rate of beds for severe patients is approximately 60%.
< Areas other than the above >
In Iwate, Miyagi, Akita, Toyama, Fukui, Yamanashi, Shiga, Nara, Wakayama, Tottori, Tokushima, Ehime, and Kochi, the number of new cases of infection is approximately 72, 151, 161, 149, 171, 289, 375, 460, 341, 189, 137, 153, and 174, respectively. In some areas, the number has increased rapidly, with a ratio to that for the previous week of more than 2. The use rate of beds is slightly more than 60% in Iwate, Shiga, and Wakayama, slightly more than 70% in Yamanashi and Nara, slightly more than 30% in Toyama, Tokushima, Ehime, and Kochi, and slightly more than 20% in Miyagi, Akita, and Tottori.
Future outlook and measures to be taken
- The number of new cases of infection nationwide is increasing rapidly, with replacement by the Omicron variant. Along with the rapid increase in the number of infected individuals due to increased opportunities for contact, such as while dining out at the end and beginning of the year, the infection is also beginning to occur at homes, workplaces, schools, medical institutions, and nursing welfare facilities, and also to spread from such places. The nighttime population is generally decreasing in the areas under priority measures, although it is increasing in some areas. The ratios of new cases for this week to that for the previous week and the effective reproduction numbers indicate a decreasing trend or a state in which the increase is halting in some areas, as well as a downward trend in the pace of the increase. However, given the characteristics of the Omicron variant and the changes in parameters such as the positive PCR test rate, the spread of infection is expected to continue nationwide, even though its pace is slowing. It is therefore necessary to take measures promptly, based on the characteristics of the Omicron variant and the current infection status.
- In many areas, the numbers of persons who are positive for the COVID-19 and in close contact with infected individuals are increasing at schools, kindergartens, nursery schools, etc. In areas where the infection is spreading, it is necessary to strengthen and thoroughly enforce basic infection prevention measures at these facilities. When providing vaccination services at shortened intervals for the general public, vaccinations need to be promoted for teachers and other staff who are working at these facilities. It is also necessary to consider securing educational opportunities through measures such as staggered attendance and online lessons, and maintaining social functions.
- At nursing welfare facilities, infection prevention measures should also be strengthened. Promotion of booster vaccinations for residents and staff, as well as aggressive testing for staff is required. For infection control and medical care at facilities, external support is important.
- Individuals infected with the Delta variant, which is more likely to cause severe symptoms, are still detected, although it is being replaced by the Omicron variant. In Okinawa, where a prevalence of infections with the Omicron variant was seen earlier than in other areas, the number of infected individuals is decreasing among young people, but continues to increase in persons in their 70s, along with a continuous increase in the number of hospitalized patients. The number of infected individuals at nursing welfare facilities is also increasing. Similar trends may be seen in other areas, in the future. Due to the rapid spread of infection, mainly among young people, the number of patients under condition monitoring and the number of home care recipients continue to increase, and systems for medical care provision system and other services for mild and moderate patients are becoming strained. In addition, the spread of infection in the elderly may increase the number of severe patients, in the future. Attention should also be given to a possible increase in the number of infected individuals requiring hospitalization, as test-positive persons with an underlying disease may require hospitalization due to disease exacerbation by the infection, even in cases where they do not have COVID-19 pneumonia.
- Each year, many cases of emergency transportation usually occur during this period. According to a status survey on cases of emergency transportation difficulties, cases of suspected non-COVID-19 have increased compared to cases of suspected COVID-19, in many municipalities. With a rapid increase in the number of cases of suspected COVID-19, cases of emergency transportation difficulties have exceeded those during the same period last year and during the spread of the infection last summer. There is already a significant burden on regular medical care, especially emergency medical care.
Findings on the characteristics of the Omicron variant
- [Infectivity/transmissibility]
It has been confirmed that compared to the Delta variant, the generation time has shortened to approximately 2 days (approximately 5 days for Delta). The doubling time and incubation period have also shortened, the risk of re-infection and secondary infection after infection has increased, and the speed of infection spread is very fast.
- [Place/route of infection]
In Japan, many cases of infection occur through the same opportunities as before (spending time indoors with insufficient ventilation, eating and drinking, etc.), and infection is considered to occur via the same routes as before (droplets, aerosol inhalation, contact infection, etc.).
- [Severity]
It has been suggested that infection with the Omicron variant may present a relatively lower risk of hospitalization and aggravation than does the Delta variant. However, the number of cases of hospitalization due to the Omicron variant infection has already increased.
- [Duration of viral shedding]
Viral shedding in individuals infected with the Omicron variant decreases over time, regardless of vaccination status. In patients with symptoms, it has been shown that the possibility of viral shedding after Day 10 (when the date of onset is regarded as Day 0) is as low as in the case of infection with the conventional strain. In patients with no symptoms, it has been shown that the possibility of viral shedding is low 8 days after the date of diagnosis.
- [Vaccine effect]
For infection with the Omicron variant, the preventive effect of a first vaccination against disease onset is markedly reduced, but its preventive effect on aggravation is maintained at a certain level. It has also been reported that booster shot improves the infection-preventing effect and hospitalization-preventing effect for infection by the Omicron variant.
Efforts based on the spread of infection with the Omicron variant
- [Test/diagnosis and surveillance in areas with a rapid spread of infection]
A test/diagnosis system and the processing of notifications to public health centers are becoming strained, and there are concerns regarding discrepancies between the published data and the actual status. It is necessary to consider effective and appropriate surveillance, in order to properly grasp the trend of occurrences. Tests and active epidemiological surveys should be prioritized based on the findings obtained thus far. Regarding free tests for people who are worried about infection and wish to undergo testing, attention should be paid to a rapid increase in demand for tests as well as test availability, and a system to ensure prioritized testing needs to be secured.
- [Monitoring system for mutant strains in Japan]
While the infection is spreading nationwide, it is necessary to maintain a surveillance system according to the local infection status, including the situation regarding replacement with the Omicron variant. For severe patients, clusters, or other applicable cases, a genome analysis should also be performed to identify variants such as the Delta variant. In addition, in some areas overseas, the number of cases of infection with the BA.2 lineage is increasing. Currently, the mainstream of the Omicron variant in Japan is the BA.1 lineage, but the BA.2 lineage has also been detected in quarantine and in Japan. Monitoring must be continued by a certain number of genome analyses. In comparison between the BA.1 and BA.2 lineages, differences in hospitalization rates are not clear at this time.
- [Measures taken by local governments]
Based on the infection status of the region and forecasts of the numbers of infected cases and severe cases, local governments must work flexibly to secure the required number of beds and healthcare professionals, secure the functions of public health centers, which are indispensable for local communities, along with support for strengthening the healthcare center system, and establish home-visit and online medical care systems for home care recipients. At that time, it is necessary to secure a system for prompt administration of oral therapeutic drugs and neutralizing antibody drugs, for patients at risk of developing severe disease, such as elderly patients and patients with underlying diseases. As patients with acute diseases other than COVID-19 who require emergency transportation often appear during the winter, attention should be given to the balance between medical care for COVID-19 and regular medical care. If the infection spreads rapidly, it is necessary to take concrete actions to ensure that people have prompt access to consultation and condition monitoring according to the infection status in the area, and to prevent a collapse of outpatient care services.
- [Reinforcement of provision of information to people who have not been vaccinated or who are eligible for booster vaccination]
It is particularly important to promote the vaccination of unvaccinated persons. Local governments are required to provide information to persons who have not been vaccinated. At the same time, booster vaccinations, which have already been started, must also be implemented steadily. The number of elderly infected individuals may continue to increase in the future. Therefore, it is necessary to further accelerate vaccinations for the elderly and other eligible persons, and also to successively provide vaccination services ahead of the original schedule for the general public as well, as much as possible.
- [Quarantine measures]
The waiting period after entering Japan has been further reduced from 10 days to 7 days. It is necessary to continue to verify future quarantine measures, while taking into account the prevalence of variants such as the Omicron variant in Japan and overseas. For individuals found to be positive by an entrance test, a whole-genome analysis should continue to be performed, to monitor the strains that are spreading overseas.
An immediate review of the business continuity plan of each local business is required
- Due to the rapid spread of infection in the region, infections among employees and their families, or withdrawal from the workplace due to close contact, are increasing, especially at medical institutions and nursing welfare facilities. Since similar situations can occur in other workplaces that are necessary for social maintenance, their business continuity plans must be inspected urgently. In addition, from the viewpoint of preventing the further spread of infection while maintaining socioeconomic activities as much as possible, the scientific findings regarding the Omicron variant were again verified, to shorten the period of condition monitoring for persons in close contact with infected individuals, and to allow local governments to further shorten the period based on the results of tests for 2 consecutive days, for persons who are necessary for social maintenance. In patients with no symptoms, the period of recuperation can be shortened. It is important to continuously and appropriately review the period of condition monitoring and the period of recuperation.
- In order to maintain social functions, attendance at workplaces and opportunities for contact must be reduced by utilizing telework, promoting the taking of time off, and through other measures. In addition, occupational booster vaccination should be actively promoted.
It is essential to widely share the current infection status with citizens and business operators, and cooperate toward preventing the spread of infection.
- Governments, business operators, and citizens need to act with an awareness that the infection, mainly the Omicron variant is still spreading, not only in areas under priority measures, but throughout Japan. In addition, booster vaccinations are effective in preventing disease aggravation/onset.
- Regarding infection with the Omicron variant, basic prevention measures are still important, and people including vaccinated individuals should continue to ensure the proper wearing of nonwoven masks, hand washing, ventilation, etc. The risk of infection becomes highest when the three Cs (crowded places, closed spaces, and close contact) overlap. However, people should avoid even a single C, as much as possible, because the Omicron variant is highly transmissible.
- Crowded places and other places with a high risk of infection must be avoided when going out. Activities with small numbers of people. When it is necessary to use restaurants, it is necessary to select a third party-certified restaurant that implements infection control measures such as good ventilation, with as few people as possible, to avoid loud noises and long hours, and to wear a mask when not eating or drinking.
- In order to protect the lives of both yourself and your family, and at the same time prevent the spread of infection by the Omicron variant, it is necessary to refrain from going out if you feel a little unwell, such as a mild fever or fatigue, and to be examined and receive tests according to government policy.
Figures (Number of new infections reported etc.) (PDF)
- Details
69th meeting of the COVID-19 advisory board of Ministry of Health, Labour and Welfare (January 26, 2022). Material 1
Evaluation of the latest infection status, etc.
Infection status
- The number of new cases of infection (by date of report) nationwide was approximately 276 per 100,000 in the last week, and the ratio of the number for this week to last week continued to increase rapidly, to 2.2. The number of new cases of infection is increasing mainly in their 20s or younger, but the proportion by age group shows a decrease in patients in their 20s, while the proportion of patients under 10 years old has increased. Of 16 prefectures to where priority measures to prevent the spread of disease are applied, 15 prefectures other than Okinawa have been continuously showing a rapid increase. In Okinawa, the ratio of the number of new infections for this week to last week is below 1. It should be noted that the number of new infections is decreasing in young people mainly in their 20s, but increasing in people in their 60s and older. In addition, there continues to be rapid increase in the number of new infections in areas other than the areas subject to priority measures. With the rapid increase in the number of new cases of infection nationwide, the number of patients receiving treatment has surged, and the number of severe cases is also on the rise.
- So-called community-acquired infections of the Omicron variant have expanded, and in many regions, replacement of the epidemic strain by the Omicron variant is progressing rapidly, although the Delta variant continues to be detected.
Effective reproduction number: On a national basis, the most recent number is above 1 at 1.37 (as of January 9). The figure is 1.45 in the Tokyo metropolitan area and 1.42 in the Kansai area.
Local trends
* The value for new cases of infection is the number of people per 100,000 among the total number for the latest week, based on reporting dates.
< Area subject to priority measures >
- Tokyo metroplitan area (Tokyo and 3 neighboring prefectures)
In Tokyo, the number of new cases of infection has increased rapidly to approximately 482, with a ratio of this week to last week of 2.5. Most are in their 20s and 30s, but those in their teens or younger are also increasing. The use rate of beds is slightly more than 30%, and the use rate of beds for severe cases is about 30%. Also in Saitama, Chiba and Kanagawa, the number of new cases of infection continued to increase, reaching approximately 254, 256, and 278, respectively. In each of these prefectures, the ratio of new cases for this week to last week increased rapidly, to above 2. The use rate of beds is about 40% in Saitama, about 30% in Chiba and slightly more than 30% in Kanagawa.
- Gunma and Niigata
In Gunma, the number of new cases of infection has increased rapidly to approximately 230, with a ratio of this week to last week of 2.4. The infected individuals are mainly in their 20s or younger. The use rate of beds is slightly more than 50%. In Niigata, the number of new cases of infection has increased rapidly to approximately 141, with a ratio of this week to last week of 1.9. The infected individuals are mainly in their 20s or younger. The use rate of beds is slightly more than 20%.
- Chukyo
In Aichi, the number of new cases of infection continued to increase rapidly to approximately 295, with a ratio of this week to last week of 2.5. The infected individuals are mainly in their 20s or younger. The use rate of beds is slightly more than 20%. In Gifu and Mie, the number of new cases of infection has increased to approximately 188 and 142, respectively. In Gifu, the ratio of new cases for this week to last week increased rapidly, to above 2. The use rate of beds is slightly more than 50% in Gifu and slightly more than 30% in Mie.
- Hiroshima,Yamaguchi and Kagawa
In Hiroshima, the number of new cases of infection continued to increase to approximately 334, with a ratio of this week to last week of 1.4. The infected individuals are mainly in their 30s or younger. The use rate of beds is approximately 40%. In Yamaguchi and Kagawa, the number of new cases of infection continued to increase to approximately 171 and 124, respectively. In Kagawa, the ratio of new cases for this week to last week increased rapidly, to above 2. The use rate of beds is about 50% in Yamaguchi, about 40% in Kagawa.
- Kumamoto, Nagasaki and Miyazaki
In Kumamoto, the number of new cases of infection continued to increase to approximately 284, with a ratio of this week to last week of 1.8. The infected individuals are mainly in their 20s or younger. The use rate of beds is slightly less than 50%. In Nagasaki and Miyazaki, the number of new cases of infection continued to increase to approximately 249 and 192, respectively. In each of these prefectures, the ratio of new cases for this week to last week increased rapidly, to above 2. The use rate of beds is slightly more than 30% in both.
- Okinawa
The number of new cases of infection for this week to last week is 0.8, which is below 1, but it must be noted that the number reported may not reflect the actual situation. At about 547 it was the highest in Japan. Newly infected patients are mainly in their 30s or younger, but those younger than 10 and those in their 60s and older are increasing. The use rate of beds is slightly more than 60%, and the use rate of beds for severe cases is slightly less than 70%.
< Other than areas subject to priority measures >
- Hokkaido
The number of new cases of infection is increasing rapidly and has reached approximately 202 (approximately 284 in Sapporo City), with a ratio of this week to last week of 2.8. The infected individuals are mainly in their 20s or younger. The use rate of beds is slightly more than 20%.
- Kansai areas
In Osaka, the number of new cases of infection continued to increase rapidly to approximately 513, with a ratio of this week to last week of 2.0. The infected individuals are mainly in their 20s or younger. The use rate of beds is about 50%, and the use rate of beds for severe cases is about 20%. In Shiga, Kyoto, Hyogo, Nara, and Wakayama, the number of new cases of infection continued to increase, reaching approximately 246, 374, 340, 248, and 213, respectively. In Kyoto, Hyogo, and Nara, the ratio of new cases for this week to last week increased rapidly, to above 2. The use rate of beds is slightly more than 40% in Shiga, slightly more than 30% in Kyoto, approximately 60% in Nara, slightly more than 40% in Hyogo, and slightly more than 70% in Wakayama. The use rate of beds for severe cases is slightly more than 20% in Kyoto and Wakayama, and slightly less than 30% in Nara.
- Kyushu
In Fukuoka, the number of new cases of infection continued to increase rapidly to approximately 350, with a ratio of this week to last week of 2.7. The infected individuals are mainly in their 20s or younger. The use rate of beds is slightly more than 20%. In Saga, Oita, and Kagoshima, the number of new cases of infection continued to increase, reaching approximately 224, 192, and 153, respectively. In Oita and Kagoshima, the ratio of new cases for this week to last week increased rapidly, to above 2. The use rate of beds is slightly more than 30% in Saga, about 40% in Oita and slightly less than 40% in Kagoshima.
- Areas other than the above
Aomori, Iwate, Miyagi, Akita, Yamagata, Fukushima, Ibaraki, Tochigi, Toyama, Ishikawa, Fukui, Yamanashi, Nagano, Shizuoka, Tottori, Shimane, Okayama, Tokushima, Ehime, and Kochi were approximately 112, 29, 71, 73, 58, 51, 142, 161, 59, 143, 100, 164, 153, 206, 114, 161, 199, 64, 135, and 90, respectively. The use rate of beds is about 20% in Aomori, and about 30% in Iwate. It is slightly less than 30% in Yamagata and Okayama, slightly less than 40% in Fukushima, Nagano and Kochi, slightly more than 20% in Ibaraki, Toyama, Shizuoka, Tottori, Tokushima and Ehime, slightly more than 30% in Tochigi, Ishikawa and Shimane, and slightly more than 50% in Yamanashi.
Future outlook and measures to be taken
- The number of new cases of infection nationwide is rapidly increasing with replacement by the Omicron variant. In addition to the 16 prefectures that have already been designated as areas subject to priority measures, priority measures will be newly applied to 18 prefectures from January 27. The rapid increase in the number of infected people was largely influenced by the increase in contact opportunities due to year-end parties, Christmas and New Year holidays, and the long weekend in January, but the sites of infection are thought to be spreading to homes, workplaces, schools, medical facilities, and long-term care facilities. The nighttime population is generally decreasing in the areas subject to priority measures, although it is increasing in some areas. From the ratio of this week to last week and the effective reproduction number, the rate of increase is slowing down, but based on the characteristics of the Omicron variant and the positive rate of PCR tests, etc., the spread of infection is expected to continue nationwide, at least in the short term, and measures based on the characteristics of the Omicron variant must be taken promptly.
- In schools, kindergartens, nursery schools, etc., the numbers of people positive for COVID-19 infection and in close contact are increasing in many areas. In areas where infection has spread, it is necessary to strengthen and thoroughly implement basic infection control measures and also to secure educational opportunities and maintain social functions at these facilities.
- Although it is being replaced by the Omicron variant, individuals infected with the Delta variant are also detected. Infection with the Delta variant is more likely to become severe, and in fact severe cases have occurred. In Okinawa, which had earlier prevalence of infection by the Omicron variant, the number of infected cases is decreasing among young people, but the number of infected cases continues to increase at the age of 60 and over, and the number of hospitalized patients continues to increase. Similar trends may be seen in other regions in the future. The rapid spread of infection mainly in young people may cause the medical care provision system for mild and moderate cases to quickly become strained, including the response to a rapid increase in health observers and home care recipients. Thereafter, the spread of infection in the elderly may lead to increase in the number of severely ill patients. Attention should also be given to increases in the number of infected patients requiring hospitalization due to an underlying disease exacerbated by the infection, even if the positive person with the underlying disease does not have pneumonia due to COVID-19 infection. Many cases of emergency transport normally occur during this period, and according to the status survey on cases of difficulty in emergency transport, not only cases of suspected COVID-19 but also cases of suspected non-COVID-19 are increasing. With a rapid increase in the number of cases of suspected COVID-19, cases of emergency transport difficulties have exceeded those during the same period last year or the spread of infection in last summer. There is already a significant burden on regular medical care, especially emergency medical care.
- Findings on the characteristics of the Omicron variant
- [Infectivity/transmissibility]
It has been confirmed that compared to the Delta variant, the generation time has shortened to approximately 2 days (approximately 5 days for Delta). The doubling time and incubation period have also shortened, the risk of re-infection and secondary infection after infection has increased, and the speed of infection spread is very fast.
- [Place/route of infection]
In Japan, many infections occur from the same opportunities as before (indoors with insufficient ventilation, opportunities of eating and drinking, etc.), and the routes of infection are considered to be via droplets, aerosol inhalation, contact infection, etc. as before.
- [Severity]
It has been suggested that infection with the Omicron variant may have a relatively lower risk of hospitalization and aggravation than the Delta variant, but in some areas, hospitalizations due to the Omicron variant infection have already increased.
- [Duration of viral shedding]
Viral shedding in patients infected with the Omicron variant decreased over time regardless of vaccination status, showing that the possibility of viral shedding is low from 10days after onset or diagnosis, as with the conventional strain.
- [Vaccine effect]
The preventive effect against infection with the Omicron variant by primary immunization is markedly reduced, but the preventive effect on aggravation is maintained at a certain level. It has also been reported that booster shot improves the infection-preventing effect and hospitalization-preventing effect for infection by the Omicron variant.
- [Infectivity/transmissibility]
- Efforts based on the spread of infection by Omicron variant
- [Test/diagnosis and surveillance in areas where infection is rapidly spreading]
The test/diagnosis system and process of notification to public health centers are becoming strained, and there is concern that the published data may differ from the actual situation. Effective and appropriate surveillance must be considered in order to understand the trends of occurrence. Tests and active epidemiological surveys should be prioritized based on the findings so far. It is necessary to actively perform tests for employees at facilities for the elderly, based on the Basic Policies for Novel Coronavirus Disease Control. In addition, it has become possible to receive free tests for those who are worried about infection and wish to receive such tests. However, attention needs to be paid to the rapid increase in the demand for these tests as well as the ability of the tests, and a system to ensure prioritized testing needs to be secured.
- [Monitoring system for mutant strains in Japan]
While the spread of infection is progressing nationwide, it is necessary to continue the surveillance system according to the local infection status, including the situation of replacement with the Omicron variant. In severe cases and cluster cases, confirmation by genome analysis, including the Delta variant, is also required. In some areas overseas, infection by the BA.2 lineage is increasing. Currently, the mainstream of the Omicron variant in Japan is the BA.1 lineage, but the BA.2 lineage has also been detected in quarantine and in Japan. Monitoring must be continued by a certain number of genome analyses. In comparison between the BA.1 and BA.2 lineages, differences in hospitalization rates are not clear at this time.
- [Measures taken by local governments]
Based on the infection status of the region and forecasts of the numbers of infected cases and severe cases, local governments must work flexibly to secure the required number of beds and healthcare professionals, secure the functions of public health centers, which are indispensable for local communities, along with support for strengthening the healthcare center system, and establish home-visit and online medical care systems for home care recipients. At that time, it is necessary to secure a system for prompt administration of oral therapeutic drugs and neutralizing antibody drugs for patients at risk of developing severe disease, such as elderly patients and patients with underlying diseases. At the same time, attention should be paid to the balance with ordinary medical care. If the infection spreads rapidly, it is necessary to promptly take concrete action for consultations and health observation according to the infection situation in the area, and prevent dysfunction in outpatient care.
- [Reinforcement of information provision to non-vaccinated and booster vaccinated people]
It is particularly important to promote the vaccination of unvaccinated people. Local governments are required to provide information to persons who have not been vaccinated. At the same time, booster vaccinations, which have already been started, must also be implemented steadily. In doing so, it is necessary to smoothly carry out an accelerated vaccination of healthcare professionals and the elderly.
- [Border control measures]
It is necessary to regard those who are positive in the immigration inspection as positive for the Omicron variant, and to continue whole-genome analysis for positives, in order to monitor strains circulating overseas. The waiting period after entering Japan has been shortened to 10 days, but it is necessary to continue to verify future border control measures, including the waiting period, while taking into account the prevalence of the Omicron variant in Japan and overseas.
- [Test/diagnosis and surveillance in areas where infection is rapidly spreading]
- Immediate review of the business continuity plan of each business in the region is necessary
- Due to the rapid spread of infection in the region, infections among employees and their families, or withdrawal from the workplace due to close contact, are increasing, especially at medical institutions and nursing welfare facilities. Since the same thing can happen in other workplaces needed for social maintenance, their business continuity plans must urgently be inspected. In addition, based on the newly obtained scientific findings on the Omicron variant, it is possible to shorten the period of health observation for healthcare professionals and close contacts, and to further shorten the period by combining tests for people needed for the maintenance of social functions, at the discretion of the region. The period of recuperation for unvaccinated people was determined to be the same as that for vaccinated individuals. The period of health observation and the period of recuperation must be continuously reviewed appropriately.
- In order to maintain social functions, the number of workers and the opportunities for contact must be reduced by using telework and promoting the taking of time off.
- It is essential to share the current infection situation widely with citizens and businesses, and cooperate to prevent the spread of infection.
- Governments, businesses, and citizens need to act with the awareness that infection, mainly with the Omicron variant, is spreading not only in areas subject to priority measures, but throughout the country.
- Basic anti-infection measures are also important for the Omicron variant, and it is necessary to continue to ensure proper wearing of nonwoven masks, hand washing, ventilation, etc., including among vaccinated people. Although the risk of infection is highest when the three Cs (crowded places, closed spaces, and close contact) overlap, even one C must be avoided as much as possible, due to the high transmissibility of the Omicron variant.
- In areas where infection has spread, it is necessary to strengthen and thoroughly implement basic infection control measures in school activities, but also to secure educational opportunities and maintain social functions.
- Crowded places and places with a high risk of infection must be avoided when going out. Activities with small numbers of people. When it is necessary to use restaurants, it is necessary to select a third party-certified restaurant that implements infection control measures such as good ventilation, with as few people as possible, to avoid loud noises and long hours, and to wear a mask when not eating or drinking.
- In order to protect the lives of both yourself and your family, and at the same time prevent the spread of infection by the Omicron variant, it is necessary to refrain from going out if you feel a little unwell, such as a mild fever or fatigue, and to be examined and receive tests according to government policy.
Figures (Number of new infections reported etc.) (PDF)
- Details
68th meeting of the COVID-19 advisory board of Ministry of Health, Labour and Welfare (January 20, 2022). Material 1
Evaluation of the latest infection status, etc.
Infection status
- The number of new cases of infection (by date of report) nationwide was approximately 147 per 100,000 in the last week, and the ratio of the number for this week to last week continued to increase rapidly, to 3.6. The number of newly infected people is increasing mainly among people in their 20s. In addition to Okinawa, Yamaguchi, and Hiroshima, where priority measures to prevent the spread of disease are being applied, the number of new cases of infection continues to increase rapidly, not only in urban areas such as in the Kanto and Kansai regions (e.g., Tokyo and Osaka), but also in other regions. With the rapid increase in the number of new cases of infection nationwide, the number of patients receiving treatment has surged, and the number of severe patients is also on the rise.
- So-called community-acquired infections of the Omicron variant have expanded, and in many regions, replacement of the epidemic strain by the Omicron variant is progressing rapidly, although the Delta variant continues to be detected
Effective reproduction number: On a national basis, the most recent number is above 1 at 1.43 (as of January 3). The figure is 1.45 in the Tokyo metropolitan area and 1.42 in the Kansai area.
Local trends
* The value for new cases of infection is the number of people per 100,000 among the total number for the latest week, based on reporting dates.
- Area subject to priority measures
The number of new cases of infection in Okinawa is 1.1 this week compared to last week, but it must be noted that the number reported may not reflect the actual situation. Furthermore, at about 673 it was the highest in Japan. Most are in their 20s or younger, but those in their teens or younger and those in their 60s or older are increasing. The use rate of beds is slightly less than 60%, and the use rate of beds for severe patients is slightly more than 60%. In Yamaguchi, the number of new cases of infection is approximately 130, and the ratio of this week to last week is 1.6. The use rate of beds is slightly more than 40%. In Hiroshima, the number of new cases of infection is approximately 257, and the ratio of this week to last week is 1.9. The use rate of beds is slightly more than 40%.
- Hokkaido
The number of new cases of infection is increasing rapidly, and has reached approximately 90 (approximately 120 in Sapporo City), with a ratio of this week to last week of 5.6. The infected individuals are mainly in their 20s or younger. The use rate of beds is slightly more than 10%.
- North Kanto
The number of new cases of infection has continued to increase in Ibaraki, Tochigi, and Gunma, reaching approximately 66, 84, and 110, respectively. In each of these prefectures, the ratio of new cases for this week to last week increased rapidly, to above 2. The use rate of beds is slightly more than 20% in Tochigi and slightly less than 40% in Gunma.
- Tokyo metropolitan area(Tokyo and 3 neighboring prefectures)
In Tokyo, the number of new cases of infection has increased rapidly to approximately 229, with a ratio of this week to last week of 4.0. The infected individuals are mainly in their 20s or younger. The use rate of beds is slightly more than 20%, and the use rate of beds for severe patients is slightly less than 20%. Also in Saitama, Chiba and Kanagawa, the number of new cases of infection continued to increase, reaching approximately 129, 123, and 124, respectively. In each of these prefectures, the ratio of new cases for this week to last week increased rapidly, to above 2. The use rate of beds is approximately 30% in Saitama, slightly more than 10% in Chiba and slightly less than 20% in Kanagawa.
- Chukyo/Tokai
In Aichi, the number of new cases of infection continued to increase rapidly to approximately 148, with a ratio of this week to last week of 4.8. The infected individuals are mainly in their 20s or younger. The use rate of beds is slightly more than 10%. In Gifu, the number of new cases of infection continued to increase rapidly to approximately 97, with a ratio of this week to last week of 4.2. In Shizuoka and Mie, the number of new cases of infection has increased to approximately 103 and 85, respectively. In each of these prefectures, the ratio of new cases for this week to last week increased rapidly, to above 2. The use rate of beds is slightly less than 30% in Gifu and slightly more than 20% in Mie.
- Kansai area
In Osaka, the number of new cases of infection continued to increase rapidly to approximately 303, with a ratio of this week to last week of 4.6. The infected individuals are mainly in their 20s or younger. The use rate of beds is slightly less than 30%. In Shiga, Kyoto, Hyogo, Nara, and Wakayama, the number of new cases of infection continued to increase, reaching approximately 149, 217, 169, 125, and 126, respectively. In each of these prefectures, the ratio of new cases for this week to last week increased rapidly, to above 2. The use rate of beds is approximately 50% in Shiga, approximately 30% in Kyoto, slightly less than 40% in Nara, slightly more than 30% in Hyogo, and slightly more than 80% in Wakayama.
- Kyushu
In Fukuoka, the number of new cases of infection continued to increase rapidly to approximately 163, with a ratio of this week to last week of 5.9. The infected individuals are mainly in their 20s or younger. The use rate of beds is approximately 10%. In Saga, Nagasaki, Kumamoto, Oita, Miyazaki, and Kagoshima, the number of new cases of infection continued to increase, reaching approximately 140, 120, 185, 88, 89, and 75, respectively. In most areas, the ratio of new cases for this week to last week increased rapidly, to more than 2. The use rate of beds is slightly less than 30% in Saga, slightly more than 20% in Nagasaki, Oita, and Kagoshima, approximately 30% in Kumamoto, and slightly less than 20% in Miyazaki.
- Area other than the above
Aomori, Miyagi, Akita, Yamagata, Niigata, Ishikawa, Fukui, Yamanashi, Nagano, Tottori, Shimane, Okayama, Tokushima, Kagawa, Ehime, and Kochi were approximately 76, 30, 25, 26, 87, 57, 59, 94, 88, 63, 117, 95, 32, 61, 100, and 38, respectively. The use rate of beds is slightly more than 20% in Niigata, Kagawa, Ehime, and Kochi, slightly more than 30% in Yamagata and Yamanashi, slightly less than 30% in Nagano, slightly more than 30% in Tottori and Shimane, and approximately 20% in Tokushima.
Future outlook and measures to be taken
- The number of newly infected people nationwide is rapidly increasing with replacement by the Omicron variant. In addition to the 3 prefectures that have already been designated as areas to priority measures, priority measures will be newly applied to Tokyo and 12 prefectures from January 21. The rapid increase in the number of infected people this time was considered to have been largely affected by the increase in the opportunities for contact due to year-end parties, Christmas, New Year holidays, and long weekend in January. However, because of the possibility that rapid expansion of infection will continue nationwide based on the characteristics of the Omicron variant, the current rate of increase in the number of infected people, and the rate of positive PCR tests, early measures are required.
- Although the Delta variant is being replaced by the Omicron variant, individuals infected with the Delta variant are also detected. Infection with the Delta variant is more likely to become severe, and in fact severe cases have occurred. The nighttime population tends to increase, especially in urban areas. If the current rapid spread of infection centered on young people continues, there is a possibility that the medical care provision system for mild and moderate cases will rapidly become strained, including the response to a rapid increase in health observers and home care recipients. In addition, the spread of infection in the elderly may lead to increase in the number of severely ill patients. Attention should also be given to the occurrence of cases that are positive for the novel coronavirus among hospitalized patients in ICU and ward settings in general medical care, and increases in the number of infected patients requiring hospitalization, as the underlying disease worsens due to infection. Therefore, the spread of infection must be controlled as soon as possible.
- Findings on the characteristics of the Omicron variant
- [Infectivity/transmissibility]
It has been confirmed that compared to the Delta variant, the generation time has shortened to approximately 2 days (approximately 5 days for Delta). The doubling time and incubation period have also shortened, the risk of re-infection and secondary infection after infection has increased, and the speed of infection spread is very fast.
- [Place/route of infection]
In Japan, many infections occur from the same opportunities as before (indoors with insufficient ventilation, opportunities of eating and drinking, etc.), and the routes of infection are considered to be via droplets, aerosol inhalation, contact infection, etc. as before.
- [Severity]
It has been suggested that infection with the Omicron variant may have a relatively lower risk of hospitalization and aggravation than the Delta variant, but in some areas, hospitalizations due to the Omicron variant infection have already increased.
- [Duration of viral shedding]
Viral shedding in patients infected with the Omicron variant decreased over time regardless of vaccination status, showing that the possibility of viral shedding is low from 10days after onset or diagnosis, as with the conventional strain.
- [Vaccine effect]
The preventive effect against infection with the Omicron variant by primary immunization is markedly reduced, but the preventive effect on aggravation is maintained at a certain level. It has also been reported that booster shot improves the infection-preventing effect and hospitalization-preventing effect for infection by the Omicron variant.
- [Infectivity/transmissibility]
- Efforts based on the spread of infection by Omicron variant
- [Monitoring system in Japan]
While the spread of infection with the Omicron variant is progressing nationwide, it is necessary to continue the surveillance system according to the local infection status, including the situation of replacement with the Omicron variant. In regions experiencing a rapid spread of infection, it is necessary to prioritize tests and active epidemiological surveys based on the findings obtained thus far, and to change the treatment systems. It is also necessary to confirm the Delta variant in severe cases and cluster cases. Monitoring must be continued by a certain number of genome analyses.
- [Measures taken by local governments]
Based on the infection status of the region and forecasts of the numbers of infected cases and severe cases, local governments must work flexibly to secure the required number of beds and healthcare professionals, secure the functions of public health centers, which are indispensable for local communities, along with support for strengthening the healthcare center system, and establish home-visit and online medical care systems for home care recipients. At that time, it is necessary to secure a system for prompt administration of oral therapeutic drugs and neutralizing antibody drugs for patients at risk of developing severe disease, such as elderly patients and patients with underlying diseases.
- [Implementation of tests]
In regions where the infection is spreading, it is necessary to actively perform tests for employees at facilities for the elderly, based on the Basic Policies for Novel Coronavirus Disease Control. In addition, it has become possible to receive free tests for those who are worried about infection and wish to receive such tests. However, in regions where the infection is spreading rapidly, attention needs to be paid to the rapid increase in the demand for these tests as well as the ability of the tests, and a system to ensure prioritized testing needs to be secured.
- [Reinforcement of information provision to non-vaccinated and booster vaccinated people]
It is particularly important to promote the vaccination of unvaccinated people, and local governments must enhance the communication of information to those who have not yet been vaccinated. At the same time, booster vaccinations, which have already been started, must also be implemented steadily. In doing so, it is necessary to smoothly carry out an accelerated vaccination of healthcare professionals and the elderly.
- [Border control measures]
It is necessary to regard those who are positive in the immigration inspection as positive for the Omicron variant, and to continue whole-genome analysis for positives, in order to monitor strains circulating overseas. The waiting period after entering Japan has been shortened to 10 days, but it is necessary to continue to verify future border control measures, including the waiting period, while taking into account the prevalence of the Omicron variant in Japan and overseas.
- [Monitoring system in Japan]
- Immediate review of the business continuity plan of each business in the region is necessary
- Due to the rapid spread of infection in the region, infections among employees and their families, or withdrawal from the workplace due to close contact is highly likely, especially at medical institutions and nursing welfare facilities. Since the same thing can happen in other workplaces needed for social maintenance, their business continuity plans must urgently be inspected. In addition, based on the newly obtained scientific findings on the Omicron variant, it is possible to shorten the period of health observation for healthcare professionals and close contacts, and to further shorten the period by combining tests for people needed for the maintenance of social functions, at the discretion of the region. The period of recuperation for unvaccinated people was determined to be the same as that for vaccinated individuals. The period of health observation and the period of recuperation must be continuously reviewed appropriately.
- It is essential to share the current infection situation widely with citizens and businesses, and cooperate to prevent the spread of infection.
- Governments, businesses, and citizens need to act with the awareness that infection with the Omicron variant is spreading not only areas in priority measures, but throughout the country.
- Basic anti-infection measures are also important for the Omicron variant, and it is necessary to continue to ensure proper wearing of masks, hand washing, ventilation, etc., including among vaccinated people. Although the risk of infection is highest when the three Cs (crowded places, closed spaces, and close contact) overlap, even one C should be avoided as much as possible, due to the high transmissibility of the Omicron variant.
- Crowded places and places with a high risk of infection must be avoided when going out. When it is necessary to use restaurants, it is necessary to select a third party-certified restaurant that implements infection control measures such as good ventilation, with as few people as possible, to avoid loud noises and long hours, and to wear a mask when not eating or drinking.
- In order to protect the lives of both yourself and your family, and at the same time prevent the spread of infection by the Omicron variant, it is necessary to refrain from going out if you feel a little unwell, such as a mild fever or fatigue, and to be examined and receive tests according to government guidelines.
Figures (Number of new infections reported etc.) (PDF)
- Details
67th meeting of the COVID-19 advisory board of Ministry of Health, Labour and Welfare (January 13, 2022). Material 1
Evaluation of the latest infection status, etc.
Infection status
- The number of new cases of infection (by date of report) nationwide was approximately 41 per 100,000 in the last week, and the ratio of the number for this week to last week continued to increase rapidly, to 8.5. The number of newly infected people is increasing rapidly, mainly among people in their 20s. In addition to Okinawa, Yamaguchi, and Hiroshima, where priority measures to prevent the spread of disease are being applied, the number of new cases of infection is increasing rapidly at an unprecedented rate, not only in urban areas such as in the Kanto and Kansai regions (e.g., Tokyo and Osaka), but also in other regions, as well. With the rapid increase in the number of new cases of infection nationwide, the number of patients receiving treatment has surged, and the number of severe patients is also on the rise.
- So-called community-acquired infections of the Omicron variant have expanded in most prefectures, and in some regions, replacement of the epidemic strain by the Omicron variant is progressing rapidly. Considering the high transmissibility of the Omicron variant, it is necessary to pay attention to the possibility that the infection will spread rapidly in the future, that the numbers of patients who are receiving treatment at home and at accommodation facilities, as well as those who require inpatient treatment will increase rapidly, and that the medical care provision system for patients with mild/moderate symptoms will be placed under severe pressure.
Effective reproduction number: On a national basis, the most recent number is above 2, at 2.29 (as of December 28). The figure is 2.27 in the Tokyo metropolitan area and 1.98 in the Kansai area.
Local trends
* The value for new cases of infection is the number of people per 100,000 among the total number for the latest week, based on reporting dates.
- Areas subject to priority measures
In Okinawa, Yamaguchi, and Hiroshima, where priority measures are being applied, the number of infected patients is continuing to increase rapidly. The number of new cases of infection in Okinawa is approximately 605, and the ratio of the number for this week to last week was 7.6, which is the highest in Japan. The infected individuals are mainly in their 20s or younger. The use rate of beds and the rate of beds for severe patients are each at slightly more than 40%. In Yamaguchi, the number of new cases of infection is approximately 81, and the ratio of this week to last week is 3.6. The use rate of beds is slightly more than 40%. In Hiroshima, the number of new cases of infection is approximately 135, and the ratio of this week to last week was 9.6. The use rate of beds is approximately 30%.
- Hokkaido
The number of new cases of infection is increasing rapidly, and has reached approximately 16 (approximately 19 in Sapporo City), with a ratio of this week to last week of 5.2. The use rate of beds is less than 10%.
- North Kanto
The number of new cases of infection has continued to increase in Ibaraki, Tochigi, and Gunma, reaching approximately 17, 25, and 36, respectively. In each of these prefectures, the ratio of new cases for this week to last week increased rapidly, to above 2. The use rate of beds is slightly less than 20% in both Tochigi and Gunma.
- Tokyo metropolitan area (Tokyo and 3 neighboring prefectures)
In Tokyo, the number of new cases of infection has increased rapidly to approximately 57, with a ratio of this week to last week of 8.5. The infected individuals are mainly in their 20s or younger. The use rate of beds is approximately 10%. In Saitama, Chiba, and Kanagawa, the number of new cases of infection has also been increasing, reaching approximately 29, 28, and 29, respectively. In each of these prefectures, the ratio of new cases for this week to last week increased rapidly, to above 2.
- Chukyo/Tokai
In Aichi, the number of new cases of infection has increased rapidly to approximately 31, with a ratio of this week to last week of 12.0. The infected individuals are mainly in their 20s or younger. The use rate of beds is less than 10%. In Gifu, the number of new cases of infection has increased rapidly to approximately 23, with a ratio of this week to last week of 6.8. In Shizuoka and Mie, the number of new cases of infection has increased to approximately 21 and 15, respectively. In each of these prefectures, the ratio of new cases for this week to last week increased rapidly, to above 2.
- Kansaia area
In Osaka, the number of new cases of infection has increased rapidly to approximately 65, with a ratio of this week to last week of 8.2. The infected individuals are mainly in their 20s or younger. The use rate of beds is slightly less than 20%. In Shiga, Kyoto, Hyogo, and Nara, the number of new cases of infection has increased to approximately 46, 52, 27, and 44, respectively. In each of these prefectures, the ratio of new cases for this week to last week increased rapidly, to above 2. The use rate of beds is slightly less than 40% in Shiga, slightly less than 30% in Kyoto, and slightly more than 20% in Nara.
- Kyushu
In Fukuoka, the number of new cases of infection has increased rapidly to approximately 28, with a ratio of this week to last week of 13.4. The infected individuals are mainly in their 20s or younger. The use rate of beds is less than 10%. In Saga, Kumamoto, and Kagoshima, the number of new cases of infection has increased to approximately 48, 31, and 48, respectively. In each of these prefectures, the ratio of new cases for this week to last week increased rapidly, to above 2.
- Areas other than the above
The numbers of new cases of infection continued to increase rapidly in nearly all other regions, especially in Niigata, Fukui, Nagano, and Shimane. The number is approximately 25, 28, 36, and 32, respectively. The use rate of beds is slightly more than 20% in Nagano and approximately 40% in Shimane.
Future outlook and measures to be taken
- In addition to Okinawa, Yamaguchi, and Hiroshima, where priority measures to prevent the spread of the disease have been applied since January 9, there has been a rapid increase in the number of new cases of infection nationwide. Furthermore, the number of patients infected with the Omicron variant has also increased, and the Delta variant has already been replaced by the Omicron variant. On the other hand, people infected with the Delta variant have also been detected, and since infection by the Delta variant is more likely to become severe, caution is necessary. As for the nighttime population, although the number decreased at the beginning of the year as a nationwide trend, it has recently started to increase once again. The rapid expansion of infection may continue in the future, considering the fact that indoor activities have been increasing with the decrease in temperature, in addition to an increase in the movement of people due to homecoming visits during the year-end and new-year holidays, and the long weekend in January, as well as increasing interactions between persons who do not usually come into contact.
- Depending on the future increasing trend, there are concerns regarding strains on the medical care provision system and the spread of infection to people who are at a high risk of becoming severely ill. Tentative information on the Omicron variant is being obtained from reports from international organizations and foreign countries, as well as domestic cases of infection. There are concerns about high transmissibility, because the Delta variant has been rapidly replaced by the Omicron variant as the epidemic strain. In addition, compared with the Delta variant, it has been confirmed that the Omicron variant shortens the generation time, doubling time, and incubation period, and the risk of secondary infection and reinfection is increased. However, thus far in Japan, many cases of infection with the Omicron variant have occurred in the same situations (such as eating and drinking) as those that are characteristic of the conventional strains and the Delta variant. There have been no findings suggestive of changes in the route of infection (such as droplet/aerosol transmission, contact infection). As for vaccines, the preventive effect obtained via primary immunization on deterioration due to infection with the Omicron variant is maintained, to a certain degree. The fact that the preventive effect of vaccination against onset is markedly reduced, and also that a booster vaccination is effective against infection with the Omicron variant have also been reported overseas. It has been suggested that infection with the Omicron variant may be less likely to become severe than with the Delta variant. However, if the number of patients receiving treatment increases rapidly due to the rapid spread of infection, primarily in young people, it should be noted that the medical care provision system for mild and moderate cases may quickly become strained, and that the spread of infection among the elderly may lead to an increase in the number of severe patients. Attention should also be given to the occurrence of cases that are positive for the novel coronavirus among hospitalized patients in ICU and ward settings, in general medical care.
- Efforts against the spread of infection with the Omicron variant are required at border-control and domestic sites.
- As measures against the Omicron variant at border control under the current circumstances, it is necessary to regard those who are positive in the immigration inspection as positive for the Omicron variant, and to continue whole-genome analysis for positives. It is necessary to continue to verify future border-control measures, while taking into account the prevalence of the Omicron variant in Japan and overseas.
- While the spread of infection with the Omicron variant is progressing in Japan, it is necessary to continue the surveillance system according to the local infection status, including the situation of replacement with the Omicron variant. In areas where infection with the Omicron variant has not been observed, early detection by thorough implementation of the testing system, prompt and active epidemiological investigations, and implementation of measures to prevent the spread of infection are necessary. In regions experiencing a rapid spread of the infection, it is necessary to consider prioritizing tests and active epidemiological surveys based on the findings obtained thus far, and to change the treatment systems.
- Based on the infection status of the region and forecasts of the numbers of infected cases and severe cases, local governments must work flexibly to secure the required number of beds and healthcare professionals, secure the functions of public health centers, which are indispensable for local communities, along with support for strengthening the healthcare center system, and establish home-visit and online medical care systems for home care recipients.
-
An immediate review of the business continuity plan of each business in the region is necessary.
Due to the rapid spread of infection in the region, infections among employees and their families, or withdrawal from the workplace due to close contact is highly likely, especially at medical institutions and nursing welfare facilities. In some regions, many healthcare professionals, such as physicians and nurses, are infected or become close contacts and are absent from work, which may result in reduced hospital functions. For this reason, it is necessary to ensure that healthcare professionals can work every day through tests, etc. even if they are close contacts with people infected with the Omicron variant. In addition, it is necessary to appropriately review the recuperation period of infected persons and the health observation period of close contacts, based on scientific knowledge. Furthermore, the same situation can occur at all workplaces that are involved in maintaining social functions, such as local governments, including healthcare centers and transportation facilities. In order to prepare for such a situation, the business continuity plan should be inspected, while taking into account the recently revised Basic Policies for Novel Coronavirus Disease Control. In addition, working from home should be encouraged in the workplace.
-
The provision of information to unvaccinated people and those receiving booster vaccinations must be strengthened.
Amidst concerns about the rapid spread of the Omicron variant, it is particularly necessary to promote the vaccination of unvaccinated people, and local governments must enhance the communication of information to those who have not yet been vaccinated. At the same time, booster vaccinations, which have already been started, must also be implemented steadily. In doing so, it is necessary to smoothly carry out an acceleration of the schedule for healthcare professionals and the elderly, who are at a high risk of becoming severely ill. In addition, the oral therapeutic drug that was approved by the fast-track system is expected to have a certain effect on preventing deterioration. Medical institutions that perform follow-up observation of patients at home are required to accelerate registration, as the institution that prescribes the oral therapeutic drug. In addition, in regions where the infection is spreading, it is necessary to actively perform tests for employees at facilities for the elderly, based on the Basic Policies for Novel Coronavirus Disease Control.
- It is necessary to widely share the assumption of the rapid spread of infection by the Omicron variant.
- Governments, businesses, and citizens need to act with the recognition that the replacement of the Delta variant with the Omicron variant is progressing in Japan, and that the spread of the infection is expected to continue.
- Based on the findings obtained thus far, basic anti-infection measures are also important for the Omicron variant, and it is necessary to continue to ensure the proper wearing of masks, hand washing, ventilation, etc., including among vaccinated people. Although the risk of infection is highest when the three Cs (crowded places, closed spaces, and close contact) overlap, even one C should be avoided as much as possible, due to the high transmissibility of the Omicron variant.
- In regions where infection with the Omicron variant has been confirmed, it has become possible to receive free tests for those who are worried about infection and wish to receive such tests. However, in regions where the infection is increasing rapidly, attention needs to be paid to the rapid increase in the demand for these tests as well as the ability of the tests, and a system to ensure prioritized testing should be secured.
-
The cooperation of citizens and businesses is crucial to prevent the spread of the infection.
In order to protect the lives of both yourself and your family, and at the same time prevent the spread of infection by the Omicron variant, it is recommended to refrain from going out if you feel a little unwell, such as a mild fever or fatigue, and to proactively be examined and receive tests. Particularly in areas where the rapid spread of infection is causing concern regarding a strain on the medical care provision system, more careful judgment and actions are required. Crowded places and places with a high risk of infection must be avoided when going out. When it is necessary to use restaurants, it is necessary to select a third party-certified restaurant that implements infection control measures such as good ventilation, with as few people as possible, to avoid loud noises and long hours, and to wear a mask when not eating or drinking.
Figures (Number of new infections reported etc.) (PDF)
- Details
66th meeting of the COVID-19 advisory board of Ministry of Health, Labour and Welfare (January 6, 2022). Material 1
Evaluation of the latest infection status, etc.
Infection status
- The number of newly infected people is increasing rapidly. The number of new cases of infection (by date of report) nationwide was about 5 per 100,000 in the last week, and the most recent week-to-week ratio was 3.26. Among the areas where the number of infected people has been increasing rapidly, it was approximately 80 per 100,000 in Okinawa, with a week-to-week ratio of 6.95, approximately 22 per 100,000 in Yamaguchi, with a week-to-week ratio of 11.11, and approximately 14 per 100,000 in Hiroshima, with a week-to-week ratio of 24.69. In addition, the number of new cases of infection has increased mainly in urban areas such as the Kanto and Kansai regions. With the rapid increase in the number of new cases of infection nationwide, the number of patients being treated and the number of severe patients are on the rise.
- The number of cases of infection with the Omicron variant is continuously increasing overseas. In Japan, infection with the Omicron variant has been confirmed in about 80% of prefectures, and there are some regions where cases of unknown infection route and no history of overseas travel continue to occur. Considering that there are some regions where the Delta variant is being replaced, it is necessary to be aware that the spread of infection might rapidly progress and the medical care provision system may become strained.
Effective reproduction number:On a national basis, the most recent number remains above 1 at 1.31 (as of December 21). The figure is 1.26 in the Tokyo metropolitan area and 1.35 in the Kansai area.
Future outlook and measures to be taken
- There is a strong possibility that infection will rapidly increase in the future. The number of new cases of infection nationwide increased rapidly from the end of the year to the beginning of the year, and the number of cases infected with the Omicron variant has also been increasing. Particularly in Osaka and Okinawa, among the cases of infection with the Omicron variant, cases unrelated to overseas travel continue to occur, and the Delta variant is already being replaced by the Omicron variant. In addition, although the nighttime population is below the level at the end of last year in a wide range of regions, the current increase in the number of infected cases still reflects the situation around Christmas. In addition to the increase in movement and contact of people due to returning home at the end and the beginning of the year, considering the 3-day weekend, coming-of-age ceremonies and related gatherings, and increased indoor activities as the temperature further decreases, there is a risk that the infection will spread further.
- Depending on the future increasing trend, there are concerns about strains on the medical care provision system and the spread of infection to people at high risk of becoming severely ill. Preliminary reports on the properties and epidemiological evaluation of the Omicron variant have been made by international organizations and other countries. Information is also being obtained from domestic cases of infection. Although information is currently limited, the epidemic strain is rapidly being replaced from the Delta variant to the Omicron variant in South Africa, the United Kingdom, etc., and there is concern about high transmissibility. Compared to the Delta variant, it has been pointed out that the Omicron variant has shortened generation time, doubling time and incubation period, and the risk of secondary infection and reinfection is increased. It has been reported that although the vaccines’ preventive effect against disease aggravation has been maintained at a certain level, the preventive effect on disease onset is markedly reduced. Laboratory evaluations have indicated that some antibody therapeutics may be less effective. Epidemiological information and laboratory studies that the Omicron variant may be less likely to become severe than the Delta variant. However, if the number of infected cases rapidly increases due to the rapid spread of infection, the number of patients requiring treatment at home, accommodation facilities for recuperation or hospitalization may rapidly increase, and the medical care provision system for mild and moderate cases may quickly become strained. If infection spreads rapidly among people at high risk of aggravation, the incidence of severe illness or death may increase.
- Preventative and agile efforts are required at borders and each site in Japan.
- As measures against the Omicron variant at border control, it is necessary to regard those who are positive in the immigration inspection as positive for the Omicron variant, to promptly identify and respond to close contacts on the airplane, and continue whole-genome analysis for positives.
- In Japan, there is a concern about rapid spread of infection by the Omicron variant, and it is necessary to continue the surveillance system. Infection with the Omicron variant has been confirmed in Japan, and early detection by thorough implementation of the testing system, prompt and active epidemiological investigation, and implementation of measures to prevent spread of infection are necessary. It is recommended that those who have shared the same space as the cases with Omicron variant infection should undergo a wide range of tests, regardless of whether they wore a mask or the duration of contact.
- Based on the infection status of the region and forecasts of the numbers of infected cases and severe cases, local governments must flexibly work to secure the required number of beds, secure support for strengthening the healthcare center system such as tests and epidemiological surveys, and establish home-visit and online medical care systems for home care recipients.
-
Immediate review of the business continuity plan of each facility in the region is needed.
Due to the rapid spread of infection in the region, infection of employees and their families or withdrawal from the workplace due to close contact is highly likely, especially in medical institutions and nursing welfare facilities. The same thing can happen at all workplaces involved in maintaining social functions, such as local governments including healthcare centers and transportation facilities. This is a business continuity plan review to prepare for such a situation. The use of telework is also required in the workplace.
-
The provision of information to unvaccinated people and those receiving booster vaccination must be reinforced.
Amid concerns about the rapid spread of the Omicron variant, it is especially necessary to promote vaccination of unvaccinated people, and local governments must enhance the communication of information to those who still have to be vaccinated. At the same time, the booster vaccination that started in December last year must also be steadily implemented. In doing so, it is necessary to smoothly carry out the acceleration of the schedule for healthcare professionals and the elderly at high risk of becoming severely ill. In addition, since specially approved oral medications can be used in patients at high risk of mild to moderate aggravation, they are expected to improve access to treatment and have a certain preventive effect on aggravation.
- It is necessary to widely share the assumption of rapid spread of infection by the Omicron variant.
- Government, businesses and citizens need to act with the recognition that the replacement of the Delta variant with the Omicron variant in Japan is progressing, and that rapid spread of infection should be assumed.
- Basic anti-infection measures are also important for the Omicron variant, and it is necessary to continue to ensure proper wearing of masks, hand washing, ventilation, etc., including among vaccinated people. Although the risk of infection is highest when the three Cs (crowded places, closed spaces, and close contact) overlap, even one C should be avoided as much as possible due to the high transmissibility of the Omicron variant.
- It is well known that in regions where infection with the Omicron variant has been confirmed, free tests are available for those who are concerned about infection and wish to have such a test.
-
The cooperation of citizens and businesses is crucial to prevent the spread of infection.
In celebrating the New Year, at annual events such as New Year's parties and coming-of-age ceremonies, when eating and drinking out, it is necessary to select a third part-certified restaurant having good ventilation, with as few people as possible, avoiding loud noises and long hours, and wearing a mask when not eating or drinking. Crowded places and places with a high risk of infection must be avoided when going out. In order to protect your own life and at the same time to prevent the spread of infection by the Omicron variant, it is recommended to refrain from going out if you feel a little unwell, such as mild fever or fatigue, and to proactively be examined and receive tests. Particularly in areas where the rapid spread of infection is causing concern about strain on the medical care provision system, more careful judgment and action are required.
Figures (Number of new infections reported etc.) (PDF)
- Details
65th meeting of the COVID-19 advisory board of Ministry of Health, Labour and Welfare (December 28, 2021). Material 1
Evaluation of the latest infection status, etc.
Infection status
- The number of new cases of infection nationwide (by the reporting date) remains at a very low level of about 1.3 per 100,000 in the most recent week, and in some regions there are days with no new cases of infection. On the other hand, in addition to increase in the number of newly infected people, mainly in urban areas, there is a temporary increase in the number of patients in some regions due to clusters at social welfare and healthcare facilities, and to cases with an unknown route of infection. The most recent week-to-week ratio was 1.51, and increase has continued for more than three weeks.
- Infection with the Omicron variant has been confirmed in multiple regions, and there have been cases where the infection route is unknown at this time, as there is no history of overseas travel.
Effective reproduction number:On a national basis, the most recent number remains above 1 at 1.21 (as of December 12). The figure is 1.22 in the Tokyo metropolitan area and 1.06 in the Kansai area.
Future outlook and measures to be taken
- Although the number of new cases of infection is still very low nationwide, the spread of infection by the Delta variant continues and is increasing. In particular, in Tokyo and Kanagawa, a week-to-week ratio of 1 or more has continued for 2 weeks or longer . The nighttime population has remained near the highest level recorded at the end of October last year in Tokyo. From now, the temperature will further decrease, and indoor activities will increase. In addition, annual events such as the New Year holidays will increase exchanges between people who do not usually meet, and as well as the movement of people going home toward the end of the year and the beginning of the year, which may rapidly spread infections. For this reason, it is necessary to refrain from activities with a high risk of infection, particularly when going home or traveling, including before and after, and limit activities to as few people as possible. Attention should be paid to understanding the trend of infections because the numbers of tests at the end and the beginning of the year are smaller than usual.
- The Omicron variation has been detected around the world and there is a rapid spread of infection that has not been seen in previous mutations. In Japan as well, it is possible that a certain scale of transmission is occurring in regions, and it should be assumed that the infection will spread rapidly.
- Preliminary reports on the properties and epidemiological evaluation of the Omicron variant have been made by international organizations and other countries. Although the information currently available is limited, the epidemic strain is rapidly being replaced from the Delta variant to the Omicron variant in South Africa, the United Kingdom, etc., and there is concern about high transmissibility. Compared to the Delta variant, it has been pointed out that the generation time, doubling time and incubation period are shortened, and the risk of secondary infection and reinfection is increased. It has been reported that although the vaccines’ preventive effect against disease aggravation has been maintained at a certain level, the preventive effect on disease onset is markedly reduced. In vitro evaluations have indicated that some antibody therapeutics may be less effective. All cases of infection with the Omicron variant that are currently being followed up in Japan are mild or asymptomatic. Overseas studies also suggest that the Omicron variant may be less likely to become severe than the Delta variant. However, if the number of infected patients rapidly increases due to the rapid spread of infection, the number of patients requiring hospitalization may rapidly increase, and the medical care provision system may quickly become strained. If infection spreads rapidly among people at high risk of aggravation, the incidence of severe illness or death may increase.
- To focus on the border-control measures against the Omicron variant and to strengthen the surveillance system in Japan, it is necessary to continue to administer PCR screening for variants and whole genome analysis of all positive individuals, particularly positive individuals who have traveled abroad, and those whose epidemiological links in Japan are not clear. In the future, infection may rapidly spread in Japan, and it is necessary to inform the citizens that the focus will be shifted from quarantine measures to domestic measures. In addition, infection with the Omicron variant has been confirmed in Japan, and early detection by thorough implementation of the testing system, prompt and active epidemiological investigation, and implementation of measures to prevent spread of infection are necessary. It is also recommended that those who have shared the same space as the cases with Omicron variant infection should undergo a wide range of tests, regardless of whether they wore a mask or the duration of contact. Moreover, it is necessary to start taking “comprehensive measures to strengthen prevention, examination and early treatment,” as well as to promote strengthening of the medical care provision system and the public health system according to the situation of infection.
- Amid concerns about the spread of the Omicron variant, it is especially necessary to promote vaccination of unvaccinated people, and local governments must enhance the communication of information to those who still have to be vaccinated. At the same time, the booster vaccination that started in December must also be steadily implemented. In doing so, it is necessary to smoothly carry out the acceleration of the schedule for healthcare professionals and the elderly at high risk of becoming seriously ill, based on the above-mentioned reinforcement measures. In addition, since specially approved oral medications can be used in patients at high risk of mild to moderate aggravation, they are expected to improve access to treatment and have a certain preventive effect on aggravation.
- Since the transmission of infection is still ongoing, attention should be paid to the spread of infection triggered by the coming year-end and New Year holidays. It is highly likely that the Omicron variant is spreading in Japan, and it is necessary to act with the recognition that rapid transmission should be assumed. Therefore, it is important to continue basic anti-infection measures such as the correct way of wearing masks, hand washing, avoiding the three Cs, and ventilation among all people, including those who are vaccinated. These basic anti-infection measures are also recommended for the Omicron variant. In regions where infection with the Omicron variant has been confirmed, free tests are available for those who are concerned about infection and wish to have such a test.
- As stated in the discussion by the chairman of the Subcommittee on COVID-19 Measures on December 23, it is necessary to avoid crowded places and places with a high risk of infection when going out. In particular, things such as homecoming and traveling must be carefully considered, in view of the trends of the Omicron variant and opportunities for contact that does not occur on a daily basis. When returning home or traveling, it is now possible to receive free tests conducted by prefectures for those who cannot be vaccinated due to health reasons or for children under 12 years old. Screening is also recommended for vaccinated individuals if they meet with someone who is not vaccinated, or who are at high risk of severe illness if infected. When eating and drinking out, it is necessary to select a third part-certified restaurant having good ventilation, with as few people as possible, avoiding loud noises and long hours, and wearing a mask when not eating or drinking. In order to protect your own life and at the same time to prevent the spread of infection with the Omicron variant, it is recommended to refrain from going out if you feel a little unwell, such as mild fever or fatigue, and to proactively be examined and receive tests.
Figures (Number of new infections reported etc.) (PDF)
- Details
January 5, 2022
Active epidemiological investigation on SARS-CoV-2 infection caused by Omicron variant (Pango lineage B.1.1.529) in Japan: preliminary report on infectious period
National Institute of Infectious Diseases Disease Control and Prevention Center, National Center for Global Health and Medicine
Coronavirus disease 2019 (COVID-19), caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), continues to cause significant morbidity and mortality globally. Since the first detection of a new SARS-CoV-2 variant belonging to the Pango lineage B.1.1.529 (Omicron variant), it has been spreading rapidly around the world. The World Health Organization classified the SARS-CoV-2 variant belonging to B.1.1.529 as a Variant of Concern (VOC) due to possible changes in viral characteristics. The Omicron variant contains a larger number of mutations in its spike protein, resulting in substantial changes in its infectivity, transmissibility and/or immune evasion capabilities and raising a serious public health concern globally.
In Japan, individuals infected with SARS-CoV-2 are hospitalized in accordance with the Infectious Diseases Control Law or the Quarantine Act. Since the evidence is lacking on the Omicron variant, individuals infected with the Omicron variant (Omicron cases) have different discharge criteria from those infected with non-Omicron variants of SARS-CoV-2 (non-Omicron cases) after November 30, 2021 in Japan. According to the criteria for discharge of Omicron cases as of January 5, 2022, they are released from medical facilities after two consecutive negative tests by nucleic acid amplification or antigen quantification methods. However, there is a concern that these discharge criteria may lead to prolonged hospitalization and increase the burden on cases, medical facilities, as well as public health centers/institutions. Therefore, it is necessary to examine the duration of virus shedding in Omicron cases in order to provide evidence to simplify the discharge criteria.
Since December 3, 2021, the National Institute of Infectious Diseases (NIID) and the Disease Control and Prevention Center within the National Center for Global Health and Medicine (NCGM/DCC) have jointly initiated an investigation on Omicron cases in collaboration with several medical facilities in Japan. Here, we examined the duration of infectious virus shedding in Omicron cases identified early in this investigation. A total of 83 respiratory specimens from 21 cases (19 vaccinees and 2 unvaccinated cases; 4 asymptomatic and 17 mild cases) were subjected to SARS-CoV-2 RNA quantification using quantitative reverse transcriptase polymerase chain reaction and virus isolation tests. The date of specimen collection for diagnosis or symptom onset was defined as day 0. The amount of viral RNA was highest on 3-6 days after diagnosis or 3-6 days after symptom onset, and then gradually decreased over time, with a marked decrease after 10 days since diagnosis or symptom onset (Figure). The positive virus isolation results showed a similar trend as the viral RNA amount, and no infectious virus in the respiratory samples was detected after 10 days since diagnosis or symptom onset (Table). These findings suggest that vaccinated Omicron cases are unlikely to shed infectious virus 10 days after diagnosis or symptom onset.
Acknowledgement
We thank the following medical facilities for their contribution in providing us with valuable patient information and samples: National Center for Global Health and Medicine, Rinku General Medical Center.
Figure. Kinetics of viral RNA amount in respiratory samples obtained from Omicron variant infected cases
(A and B) Quantitative reverse transcriptase polymerase chain reaction (RT-qPCR) done at NIID for all respiratory samples received using NIID-N2 primer/probe set for cases of SARS-CoV-2 Omicron variant infection. The levels of viral RNA by (A) days since diagnosis or (B) days since symptom onset. Red bars indicate median Cq value with interquartile range. Dotted line indicates a cutoff value.
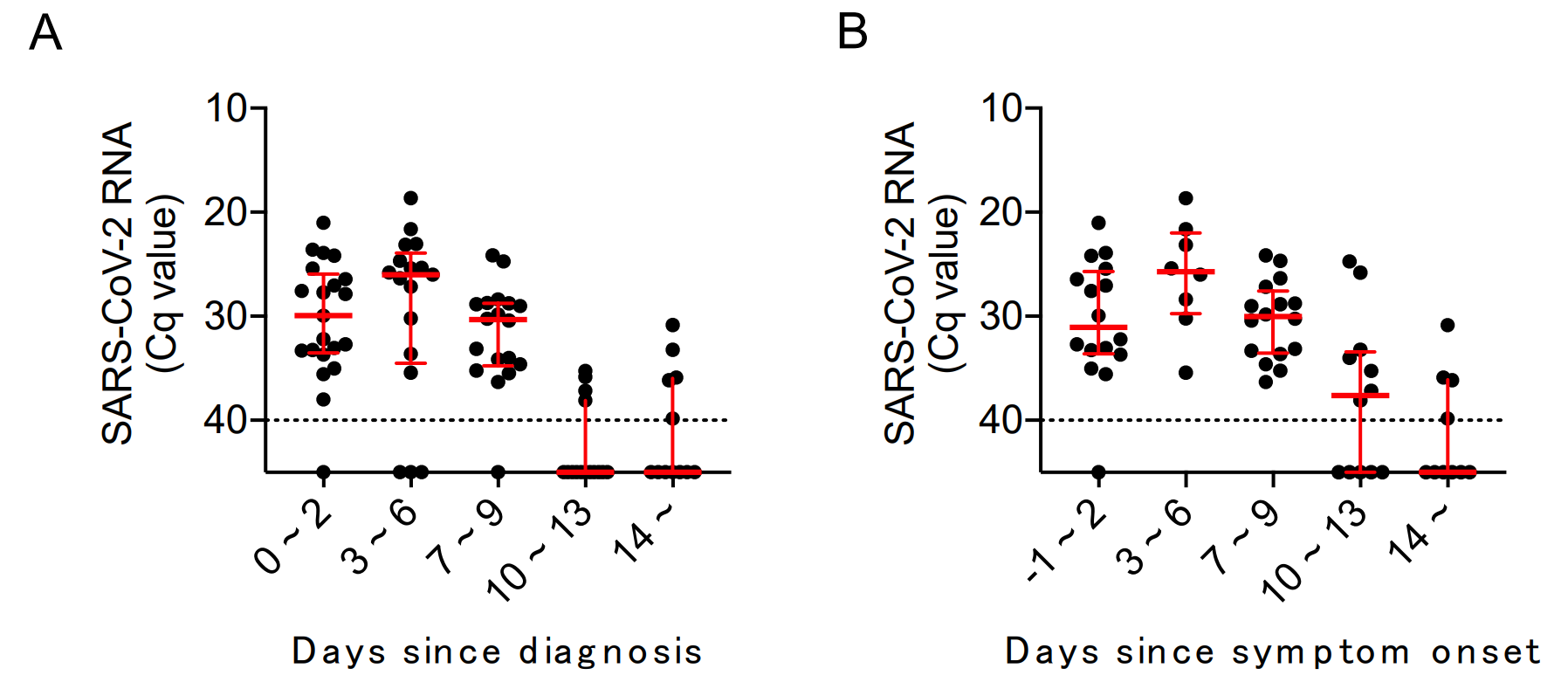
(A) Number and percentage of viral RNA positive or virus isolation positive samples by days since diagnosis
|
Days since diagnosis |
Number and percentage of viral RNA positive samples n (%) |
Number and percentage of virus isolation positive samples n (%) |
Number and percentage of virus isolation positive in viral RNA positive samples n (%) |
|
0 ~ 2 days |
20/21 (95.2) |
2/21 (9.5) |
2/20 (10.0) |
|
3 ~ 6 days |
14/17 (82.4) |
7/17 (41.2) |
7/14 (50.0) |
|
7 ~ 9 days |
17/18 (94.4) |
2/18 (11.1) |
2/17 (11.8) |
|
10 ~ 13 days |
4/15 (26.7) |
0/15 (0) |
0/4 (0) |
|
After 14 days |
5/12 (41.7) |
0/12 (0) |
0/5 (0) |
(B) Number and percentage of viral RNA positive or virus isolation positive samples by days since symptom onset (symptomatic cases only)
|
Days since symptom onset |
Number and percentage of viral RNA positive samples n (%) |
Number and percentage of virus isolation positive samples n (%) |
Number and percentage of virus isolation positive in viral RNA positive samples n (%) |
|
-1 ~ 2 days |
15/16 (93.8) |
2/16 (12.5) |
2/15 (13.3) |
|
3 ~ 6 days |
8/8 (100) |
4/8 (50.0) |
4/8 (50.0) |
|
7 ~ 9 days |
16/16 (100) |
3/16 (18.8) |
3/16 (18.8) |
|
10 ~ 13 days |
7/12 (58.3) |
0/12 (0) |
0/7 (0) |
|
After 14 days |
4/10 (40.0) |
0/10 (0) |
0/4 (0) |
(C) Number and percentage of viral RNA positive or virus isolation positive samples by days since diagnosis (asymptomatic cases only)
|
Days since positive test |
Number and percentage of viral RNA positive samples n (%) |
Number and percentage of virus isolation positive samples n (%) |
Number and percentage of virus isolation positive in viral RNA positive samples n (%) |
|
0 ~ 5 days |
6/6 (100) |
3/6 (50.0) |
3/6 (50.0) |
|
6 ~ 9 days |
3/4 (75.0) |
0/4 (0) |
0/3 (0) |
|
After 10 days |
1/10 (10) |
0/10 (0) |
0/1 (0) |
- Details
64th meeting of the COVID-19 advisory board of Ministry of Health, Labour and Welfare (December 22, 2021). Material 1
Evaluation of the latest infection status, etc.
Infection status
- The number of new cases of infection nationwide (by the reporting date) remains at a very low level of about 0.9 per 100,000 in the most recent week, and in some regions there continue to be days with no new cases of infection. On the other hand, there are some areas where the spread of infection is still ongoing. In addition, there is a temporary increase in the number of patients in some regions due to clusters at the workplace, social welfare facilities, and primary schools, as well as the occurrence of cases with an unknown route of infection. The most recent week increased from the previous week to 1.35, with 1 or more continuing for more than 2 weeks.
Effective reproduction number:On a national basis, the most recent number is above 1 at 1.11 (as of December 5). The figure is 1.23 in the Tokyo metro area and 1.02 in the Kansai area.
Future outlook and measures to be taken
- Since the Omicron variant was first reported to WHO from South Africa on November 24, cases of infection have been reported in many countries and so-called community-acquired infection has been confirmed in several countries. In Japan, genomic analysis has confirmed that many of those who tested positive for corona virus at border-control on return to Japan had the Omicron variant. In addition, the Omicron variant was confirmed in three people who had no history of overseas travel, and whose relationship with identified cases of the Omicron variant has not been confirmed. In the future, it should be assumed that the infection will spread rapidly.
- Although experimental evaluation of the properties and epidemiological information on the Omicron variant are limited, announcements and preprint article from WHO and various countries indicate high infectivity/transmissibility, risk of re-infection, and potential reduction of the preventive effect of vaccines or the effect of some therapeutic drugs. On the other hand, despite the lack of sufficient knowledge regarding its severity, we must be aware of the possibility that the medical care provision system will be suddenly strained due to the rapid spread of infection.
- To focus on the border-control measures against the Omicron variant and to strengthen the surveillance system in Japan, it is necessary to continue to administer PCR screening for variants and whole genome analysis of all positive individuals, particularly positive individuals who have traveled abroad. It is also necessary to continue to collect and analyze WHO and overseas trends, as well as clinical, epidemiological, and virological information. Based on evaluation of the infectivity, severity, and impact on vaccine efficacy of the Omicron variant by the National Institute of Infectious Diseases, as well as the status of occurrence in Japan, it will be necessary to inform the citizens of the need to shift the focus from border measures to domestic measures, in order to prevent the rapid spread of infection in Japan. In addition, when cases of infection caused by the Omicron variant occur in Japan, it is recommended that those who shared the same space as the cases with Omicron variant infection should undergo a wide range of tests regardless of whether they wore a mask or the duration of contact. Moreover, it is necessary to start taking “comprehensive measures to strengthen prevention, examination and early treatment,” including the government’s recent acceleration of vaccination, start of oral therapeutic drugs and strengthening of the examination system, as well as to promote strengthening of the medical care provision system and the public health system according to the situation of infection.
- The number of new cases of infection is still very low across the country, but is increasing. The nighttime population is also increasing, not only in urban areas but over wide areas. The nighttime population in Tokyo in particular is near the highest recorded level at the end of the last October. From now, the temperature will further decrease, and indoor activities will increase. In addition, annual vents such as year-end parties, Christmas and New Year holidays will increase exchanges between people who do not usually meet, and as well as the movement of people going home toward the end of the year and the beginning of the year, which may rapidly spread infections. For this reason, it is necessary to refrain from activities with a high risk of infection, and limit activities to as few people as possible.
- Amid concerns about the spread of the Omicron variant, it is especially necessary to promote vaccination of unvaccinated people, and local governments must enhance the communication of information to those who still have to be vaccinated. At the same time, the booster vaccination that started in December must also be steadily implemented. In doing so, it is necessary to smoothly carry out the acceleration of the schedule for healthcare professionals and the elderly at high risk of becoming seriously ill, based on the above-mentioned reinforcement measures.
- The transmission of infection by the Delta variant is still ongoing, and attention should be paid to the spread of infection triggered by the coming year-end and New Year holidays. It is also necessary to act with the recognition that the spread of the Omicron variant in Japan should be assumed. Therefore, it is important to continue basic anti-infection measures such as the correct way of wearing masks, hand washing, avoiding the three Cs, and ventilation among all people, including those who are vaccinated. These basic anti-infection measures are also recommended for the Omicron variant. It is also important to refrain from going out and proactively see a doctor if even slightly ill, such as with mild fever or fatigue, to undergo the necessary examinations. It is also necessary to select third party-certified restaurants when eating and drinking out, to wear a mask when not eating or drinking, and to avoid crowded places with a high risk of infection when going out. In particular, considering that homecoming and travel create opportunities for contacts that do not occur on a daily basis, in addition to receiving free tests in prefectures for those who cannot get vaccinated, people must refrain from traveling across prefectures when symptoms such as fever are present.
Figures (Number of new infections reported etc.) (PDF)
- Details
63th meeting of the COVID-19 advisory board of Ministry of Health, Labour and Welfare (December 16, 2021). Material 1
Evaluation of the latest infection status, etc.
Infection status
- The number of new cases of infection nationwide (based on the date of reporting) has been decreasing, and the number per 100,000 population has been approximately 0.7 in the last week, the lowest since the summer last year. However, the ratio of this week to last week was 1.17, keeping an upward trend. The numbers of patients receiving treatment, severe patients, and deaths continue to be at a low level.
Effective reproduction number:On a national basis, the most recent number remains below 1 at 0.96 (as of November 28), with values of 1.01 in the Tokyo metro area and 0.90 in the Kansai area.
Future outlook and measures to be taken
- Since the Omicron variant was first reported to WHO from South Africa on November 24, cases of infection have been reported in many countries and so-called community-acquired infection has been confirmed in several countries. By December 15, genomic analysis has confirmed that 32 of those who tested positive for corona virus at border-control on return to Japan, had the Omicron variant. Although experimental evaluation of the properties and epidemiological information on the Omicron variant are limited, there is concern about the high infectivity/transmissibility, the risk of reinfection, and its effects on vaccines and therapeutic drugs. Sufficient information on its severity has also not been obtained. To focus on the border-control measures against the Omicron variant and to strengthen the surveillance system in Japan, it is required to administer PCR screening for variants and reinforce whole genome analysis of all positive individuals, particularly positive individuals who have traveled abroad. It is also necessary to continue to collect and analyze WHO and overseas trends, as well as clinical, epidemiological, and virological information, and to take appropriate measures based on evaluation of the infectivity, severity, and impact on vaccine efficacy of the Omicron variant by the National Institute of Infectious Diseases. In addition, when cases of infection caused by the Omicron variant occur in Japan, it is recommended that those who shared the same space as the cases with Omicron variant infection should undergo a wide range of tests regardless of whether they wore a mask or the duration of contact.
- The number of new cases of infection nationwide is at a very low level, and some regions continue to see no new cases of infection. On the other hand, there are some areas where the spread of infection is still ongoing. In addition, there is a temporary increase in the number of patients in some regions due to clusters at the workplace, social welfare facilities, and primary schools, as well as the occurrence of cases with an unknown route of infection. The nighttime population is also increasing, not only in urban areas but over wide areas. The nighttime population in Tokyo in particular has increased to the highest recorded level at the end of the last October. Indoor activities will increase as it gets colder towards the end of the year, and annual events such as year-end parties and the Christmas and New Year holidays bring opportunities to have interaction with people who do not usually contact each other, and socioeconomic activities are also expected to increase. Therefore, it is necessary to carefully monitor the number of infected patients in the days ahead.
- Approximately 78% of the country's population has been fully vaccinated with two doses, and approximately 73% of those aged 12 to 19 years have been vaccinated with two doses. To further increase the vaccination rates, it is necessary to promote vaccination of unvaccinated people, and local governments must enhance the communication of information to those who still have to be vaccinated. It is also necessary to steadily implement additional vaccinations, starting in December, for those who wish to receive it.
- The infection is still being transmitted, and attention should be paid to the future spread of infection. Therefore, it is important to continue basic anti-infection measures such as the correct way of wearing masks, hand washing, avoiding the three Cs, and ventilation among all people, including those who are vaccinated. These basic anti-infection measures are also recommended for the Omicron variant. It is also necessary to select third party-certified restaurants when eating or drinking, to wear a mask when not eating or drinking, and to avoid crowded places with a high risk of infection when going out. In particular, considering that homecoming and travel create opportunities for contacts that do not occur on a daily basis, people must refrain from traveling across prefectures when symptoms such as fever are present. It is also important to proactively see a doctor for symptoms such as mild fever and fatigue to undergo the necessary examinations.
Figures (Number of new infections reported etc.) (PDF)
- Details
62th meeting of the COVID-19 advisory board of Ministry of Health, Labour and Welfare (December 8, 2021). Material 1
Evaluation of the latest infection status, etc.
Infection status
- The number of new cases of infection nationwide (based on the date of reporting) has been decreasing, and the number per 100,000 population has been approximately 0.6 in the last week, the lowest since the summer of last year. However, the ratio of this week to last week was 1.11, showing an upward trend. The numbers of patients receiving treatment, severe patients, and deaths continue to be at a low level.
Effective reproduction number:On a national basis, the most recent number remains below 1 at 0.87 (as of November 21), with values of 0.91 in the Tokyo metro area and 0.74 in the Kansai area.
Future outlook and measures to be taken
- Patients infected with the new variant (Omicron variant) have been reported in 57 countries including the United States and European countries by December 7 according to WHO, which raises concerns about the spread of the infection. Genomic analysis also confirmed the Omicron variant in 3 persons from overseas who were found to be positive for corona virus during quarantine. Although there is no experimental evaluation of the properties of the Omicron variant or sufficient information for epidemiological evaluation, there are concerns about the high infectivity/transmissibility, the risk of reinfection, and its effects on vaccines and therapeutic drugs. Sufficient information on severity has not been also obtained. To focus on the border-control measures against the Omicron variant and to strengthen the surveillance system in Japan, it is required to administer PCR screening for variants and reinforce whole genome analysis of all positive individuals, particularly positive individuals who have traveled abroad. It is also necessary to continue to collect and analyze WHO and overseas trends, as well as clinical, epidemiological, and virological information, and to take appropriate measures based on evaluation of the infectivity, severity, and impact on vaccine efficacy of the Omicron variant by the National Institute of Infectious Diseases.
- Although the number of new cases of infection nationwide is at a very low level, the spread of infection is still ongoing. In some regions, there is a temporary increase due to clusters at the workplace and in social welfare facilities, as well as the occurrence of cases with an unknown route of infection. There is therefore concern that the decreasing trend may stop. There are also regions where the nighttime population is increasing, especially in urban areas. Indoor activities will increase as it gets colder towards the end of the year, and annual events such as year-end parties and the Christmas and new year holidays, are expected to cause a further increase in socioeconomic activities. Therefore, it is necessary to carefully monitor the number of infected patients in the days ahead.
- Approximately 77% of the country's population has been fully vaccinated with two doses, and approximately 72% of those aged 12 to 19 years have been vaccinated with two dose. To further increase the vaccination rates, it is necessary to promote vaccination of unvaccinated people, and local governments must enhance the communication of information to those who still have to be vaccinated. It is also necessary to steadily implement additional vaccination, starting in December, for those who wish to receive it.
- Although the infection transmission level is low, it is still ongoing and attention should be paid to the spread of infection in the future. Therefore, it is important to continue basic anti-infection measures such as the correct wearing of masks, hand washing, avoiding the three Cs, and ventilation among all people, including those who are vaccinated. These basic anti-infection measures are also recommended for the Omicron variant. It is expected that opportunities for eating and drinking such as year-end parties will increase towards the end of the year. On such occasions, it is necessary to select third party-certified restaurants when eating or drinking, to wear a mask when not eating or drinking, and to avoid crowded places with a high risk of infection when going out. In particular, considering that homecoming and travel provide opportunities for contacts that do not occur on a daily basis, people must refrain from traveling across prefectures when symptoms such as fever are present. It is also important to proactively see a doctor for symptoms such as mild fever and fatigue to undergo the necessary examinations.
- To prevent the spread of infection, it is necessary to thoroughly implement active epidemiological studies on cases of an unknown route of infection. In addition, active measures using a broad range of tests are required for infection control at social welfare facilities and medical institutions.
Figures (Number of new infections reported etc.) (PDF)